
Analyzing Factors Responsible for Leadership Gap in Healthcare System: Suggesting Viable Solutions
December 21, 2020
Improving Occupants Safety in High Rise Buildings: Everything You Need to Know About Fire Safety
December 21, 2020
Patient Satisfaction among adult cancer patients in oncology wards in the Kingdom of Saudi Arabia (KSA)
1.1 Introduction
In the current study, patient satisfaction is examined as an aspect of patient experience and as an indicator of the quality of care among adult cancer patients in oncology wards in the Kingdom of Saudi Arabia (KSA). The aim of the current sequential mixed-methods study is to assess patient satisfaction (a characteristic of patient experience) primarily as an indicator of the quality of care among adult cancer patients in oncology wards at the Saudi Regional Cancer Centre in Riyadh (SRCC), in the Kingdom of Saudi Arabia. To do this, an MMR was used, including both formal quantitative research instruments (questionnaires) and qualitative, one-to-one interviews with patients.
Patient satisfaction is widely accepted to be an important aspect of the patient experience (Cleary et al.1989; Fitzpatrick 1991; Carr-Hill 1992; Stizia and Wood 1997; Stewart 2001; Copnell et al.2009). Patient satisfaction has always been a priority issue for health care authorities in the Saudi region evident from the recent initiative taken by the Saudi health setup to achieve “Joint Commission International (JCI)” accreditation which has further increased the importance of patient satisfaction (Alturki and Khan 2013). Patient satisfaction has been attributed to a range of factors, in particular interpersonal and structural factors (Donabedian 1980).
A core part of patient satisfaction relates to the quality of care provided by the healthcare provider (Donabedian 1980). Quality of care can be defined as access to necessary, effective health structures and service processes. Patient satisfaction with the quality of care correlates, in turn, with clinical effectiveness. That is, patient satisfaction largely depends on the confluence of healthcare providers’ practices, skills and competence, in specific contexts of time and location. The objective of these practices is to improve the patient experience to provide satisfaction through improving the quality of care to attain positive outcomes from healthcare delivery. Interpersonal factors that can have a significant influence on patient satisfaction include the nurses’ and doctors’ communication with patients, whilst significant structural factors include the size of the hospital and ward (Donabedian 1980).
Despite the acknowledged importance of patient satisfaction to patient experience, it is difficult to isolate and measure. Studies such as those by Hobb (2009) and Jagosh et al. (2011) indicate that there is no one-size-fits-all concept of patient satisfaction, due to its relativity and localisation.
The issue of quality of care has been developed as part of the recent emphasis on the systematic assessment of health care services performance across the globe (Groene et al, 2008). A key goal of improvement initiatives is to enhance patients’ experiences of health services. Derived from this concept is an aspect of patient experience; patient satisfaction which is of particular interest to the current study, specifically satisfaction attained by patients for the quality of care they receive.
Although researchers disagree on which indicators of healthcare quality are most valid, the most frequently cited dimensions of quality of care include safety, effectiveness, equity, efficiency, timeliness, and patient-centredness (IOM 2001; Doyle et al.2013 Beattie et al. 2014). The last of these, patient-centredness, has developed as a particularly fruitful area of inquiry, with researchers discovering that the doctor-patient relationship can be therapeutic (Krupat et al. 2001; Street et al. 2009; Kenny et al. 2010), and that patients’ religious/spiritual needs should be integrated into their treatment (Williamson and Harrisons 2010). However, it must be noted that on the other hand, patient-centredness does not necessarily guarantee patient satisfaction (Kupfer and Bond 2012).
In the context of the KSA, the measurement of healthcare quality in general and of patient satisfaction, in particular, is even more complicated than in Western nations. This is because the models for assessing healthcare were developed in and for Western healthcare systems (particularly in Europe and North America) and they do not translate neatly to the KSA. However, the KSA’s healthcare system is at present growing increasingly Westernized, although the residue of the old system persists—including a subordinate role for women, language barriers between providers and patients, and the practice of limiting information disclosure to patients (Younge et al 1997; Al-Shahri 2002). The main areas of the Westernization of the KSA healthcare system include health policy, standards of care, and the education of healthcare providers. In addition, KSA hospitals are seeking accreditation from major international bodies. The World Health Organization is targeting health improvement in the KSA, and the health sector is collaborating with international bodies such as international research centres and the academic sector (WHO 2009; Al-Khenizan and Shaw 2011; Al-Malki 2011). Thus, to a significant extent in this new environment, it is now possible to explore the measures of patient satisfaction that were derived in the West in the context of the KSA. Indeed, there are certain features of the KSA’s healthcare system that make this issue both urgent and complex, since they can significantly impact the quality of care. Three key features are gender politics, non-disclosure practices, and language barriers between providers and patients.


1.2 Aims of the study and research questions
The aim of this sequential mixed-methods study was to assess patient satisfaction; an aspect of patient experience, primarily as an indicator of the quality of care among adult cancer patients in oncology wards at the Saudi Regional Cancer Centre in Riyadh (SRCC), in the Kingdom of Saudi Arabia. Throughout the current study, clinical effectiveness is emphasised to comprehend the patient experience of their healthcare within oncology wards in SRCC.
The main research question emergent from this primary aim was to explore: What factors contribute to or hinder patient satisfaction with care in the oncology wards setting in the SRCC?
The specific aims of the research were as follows:
- To determine the likelihood that clinical effectiveness is associated with patient satisfaction in adult oncology ward settings in SRCC.
- To determine how likely the accessibility to health care is associated with patient satisfaction in adult oncology ward settings in SRCC.
- To describe the characteristics of patients in adult oncology ward settings in SRCC.
- To explore the extent to which interpersonal aspects of care influence patient satisfaction in adult oncology ward settings in SRCC.
- To provide recommendations for enhancing patient satisfaction in oncology ward settings in KSA.
- To discuss the extent to which and in what ways the qualitative findings help to explain the initial quantitative results of patient satisfaction in oncology settings in KSA.
The specific sub-questions formulated to achieve the specific aims of the study are as follows:
- Does the clinical effectiveness of health care (doctors’ and nurses’ skills, information provision, availability) influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
- Does accessibility to health care (service organisation) influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
- What are the socio-demographic characteristics of adult oncology inpatients at the SRCC in Riyadh?
- How do interpersonal aspects of care influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
- How do socio-cultural communication factors influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
1.3 The significance of the research
This research is significant in the following ways:
(a) The current study is one of the first in the context of the KSA to use a patient experience within a hospital context to investigate patient satisfaction;
(b) Outside a Western context (Western Europe and North America) there has been little research conducted internationally on patient satisfaction using the mixed methods approach (Merkouris et al. 2004); Hyrkas 2003).
(c) By illuminating the doctor-patient and nurse-patient relationship in the KSA, the current study contributes to the understanding of how these relationships operate in the Gulf Cooperation Council (GCC); which includes Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates, and other Arab countries (in relation to religious beliefs, cultural beliefs and patriarchal culture).
The current study will be able to influence future practices, education, and research on patient satisfaction and experiences that are held with healthcare providers in oncology wards throughout the Kingdom of Saudi Arabia.
1.4 Patient satisfaction and quality of :
This section clarifies how key terms were defined using a combination of Donabedian 1980 and Quality Dimensions 6 aims OF IOM as the prime source of definitions to quality, including quality of care, clinical effectiveness, patient experience, and patient satisfaction
1.4.1 Quality of care
Quality of care is a multi-dimensional concept that can be studied from a number of different perspectives (Chassin and Gavin 1998; Heath et al. 2009). For the current study, quality of care is defined and analysed using a combination of the Donabedian model (1980) and the Institute of Medicines Six dimensions of care. Campbell et al. (2000, p. 1614) define the quality of care as ‘whether individuals can access the health structures and processes of care which they need and whether the care received is effective’, whilst for Lohr (1990) it is ‘the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge (Lohr 1990, p.65).
Quality of care can be divided into different dimensions according to the aspects of care being assessed. Donabedian’s (1980) seminal framework for defining quality of care in healthcare settings has three components: structure, process, and outcomes. Structural components include the context in which care is delivered (including facilities, equipment, and organizational characteristics). Process components include all the actions that makeup healthcare (such as diagnosis and treatment). And outcome components include all the effects of healthcare on patients or populations. The Donabedian care-assessment model has been widely used in international healthcare settings to assess patient satisfaction with the quality of care (Ware et al.1989; Campbell et al. 2000; Kringos et al. 2010; Khamis and Njau 2014). The model is an important component of the current study’s framework.
The Institute of Medicine (IOM) (2001) devise six dimensions of health care quality known categorically as; safe, effective, patient-centred, timely, efficient, and equitable. Based on these dimensions, safe includes avoiding harm to patients from the care that is proposed to help them; effective include the provision of services that has their foundation in scientific knowledge to all who could benefit and restrain from providing services to those not likely to benefit which means avoiding the underuse and misuse of resources; patient-centred means providing care that is respectful of and responsive to individual patient preferences, needs, and values and making sure that patients’ values are the ones guiding all the clinical decisions made; timely means the reduction of wait and often harmful delays for both those who receive and give care; efficient is avoiding waste of resources such as equipment, supplies, ideas, and energy; lastly, equitable is providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, location, and socio-economic status.
Based on the analysis of both forms of measuring the quality of care the Donabedian’s model (1980) and IOM’s (2001) dimensions of care can be combined to measure and assess the quality of care more efficiently. Each of the Donabedian’s categories of structure, process and outcome can be subdivided to include the six dimensions of quality to ensure that each of the stages was executed effectively to derive inferences about the quality of care in the oncology ward setting in KSA in the current study.
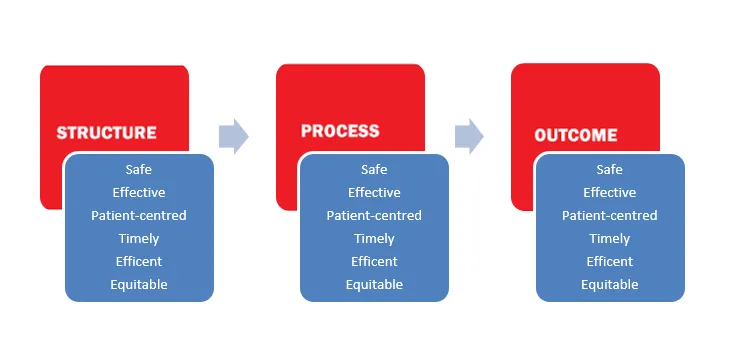
Figure 1- Combination of Donabedian' Model of care and IOM's 6 dimensions of care
1.4.2 Clinical effectiveness
The construct of clinical effectiveness is closely related to the quality of care and patient experience but refers specifically to the efficacy of care delivered by practitioners. Clinical effectiveness can be defined as ‘the right person doing the right thing (evidence-based practice) in the right way (skills and competence) at the right time (providing treatment and service when a patient needs them), in the right place (location of treatment and service) with the right result (clinical effectiveness/health gain’ (NHS QIS 2005). Methods for measuring and assessing clinical effectiveness are discussed further in Chapter 2. The evidence found in the literature suggests that there is a positive association between patient experience and clinical effectiveness (Doyle et al. 2013). In the context of the KSA, there is a lack of evidence of assessment of patient experience including satisfaction from the clinical effectiveness perspective.
1.4.3 Patient experience and patient satisfaction
Currently, patient experience is recognized as one of the crucial pillars of quality of care (Tsianakas et al.2012; Beattie et al. 2015) which is generally defined as the patient’s experience of the healthcare process impacted by the extent and assurance of quality developed through clinical effectiveness. One aspect of patient experience is the construct at the heart of the current study specifically, patient satisfaction. In general, patient satisfaction is defined as a health care recipient’s reaction to salient aspects of context, process and results of their service experience’ (Pascoe 1983 p.186). Patient satisfaction is inextricably linked to the quality of care (Cleary et al. 1989; Stewart 2001; Batbaatar et al. 2015). Patient satisfaction is an important indicator of quality care, although the formal assessment of such satisfaction is always going to be complex (Cleary 1998; Al-Rubaiee 2011). Several variant factors have an impact on specific patients and their responses to the quality of their healthcare, including their characteristics, attitudes, and prior experience (Oberst 1984; Blanchard et al.1990). A hospital may be well organised, ideally located, and well-equipped, but low patient satisfaction may still indicate it is failing to provide effective healthcare (Donabedian 1988; Draper et al. 2001; Turhal et al. 2002; Barlesi et al. 2005).
The enhancement of patient experiences of healthcare services is a key goal of improvement initiatives (Umar et al. 1995; Alturki and Khan 2013; Mohamed et al. 2015). Although the concept of patient satisfaction is complex and difficult to measure in terms of healthcare, patient surveys and self-reported outcomes have been successfully used in hospitals. They are perceived as the best quality indicator tools in hospital-based care settings (Ervin 2006; Lynn et al. 2007; Groene et al. 2008; Copnell et al. 2009). Although there is evidence of success found in self-reported outcomes, various studies (Sait et al., 2014, Stavropoulou, 2010; Al-Sakkak, 2008) have reported that many patients report satisfaction with ineffective care allotted to them. Al-Sakkak (2008) and Stavropoulou (2010) assert that many patient experience surveys may indicate satisfaction with ineffective care due to the literacy of patients being low and inadequately understanding the survey to provide an opinion on the quality of healthcare they received.
Self-reported studies of patient satisfaction are usually conducted through hospital self-assessment. This method of measuring patient satisfaction uses a set of devised questions which assesses the functions, procedures, and capability of the hospital infrastructure, staff, and policies. The results of the hospital assessment survey are then used to measure the delivery of health care and predict patient satisfaction. Patient satisfaction questionnaire forms are an instrument used to measure patient satisfaction with a set of questions that ask the patient to comment with their opinion on the healthcare that has been provided to them. Other patient satisfaction surveys are distributed to medical professionals, such as doctors and nurses to receive their opinion on the perceived level of satisfaction of patients towards health care delivery. The current study uses a patient satisfaction questionnaire, however, it differentiates from other research taken place in KSA, as viewed in the literature review in Chapter 2, as the current study uses patients within the oncology ward setting to extract information in regards to health care delivery they are experiencing instead of the use of medical professionals such as doctors.
The literature review in Chapter 2 discusses in detail ‘satisfaction’ and other methods to measure and assess patient healthcare experience as well as a discussion on various factors that may affect patient satisfaction. In particular, there appears to be evidence indicating a relationship between satisfaction and patients’ adherence to medical regimens, along with patients’ compliance with cancer treatment and improvement in health status (Ware and Davies 1983; Borras et al 2001; Westaway et al. 2003).
1.5 Overview of the study context
1.5.1 History and background of the Kingdom of Saudi Arabia
The Kingdom of Saudi Arabia was unified and established as an Islamic state in 1932. The presence of the two holy mosques (Makkah and Madinah) within the country means that the KSA has an influential political role in the Middle East and the wider Muslim world. The 2010 census found that the KSA had a population of 29.9 million, of whom 73% were Saudi citizens (Central Department of Statistics and Information, KSA 2010). There is substantial employment of non-Saudis in a number of sectors, including healthcare.
Riyadh is the capital and the largest city in the KSA. The population of Riyadh is just over 7 million, which accounts for 24% of the population of the Kingdom (World Population Review 2014). To place this in context, and to encourage an appreciation for how large this city is, the city has a population of almost 2 million more than the population of Scotland, which currently stands at just over 5 million (Scotland National Statistics 2014).
Religion is an important aspect of Saudi society and the culture and social norms are drawn from the Sunnah (a set of documents held to represent a model of life, detailing the actions and the sayings of the Prophet Muhammad ﷺ [peace be upon him, pbuh]). In effect, observant words and actions ensure that daily life fits the teachings of the Prophet of Islam, Muhammad. Specifically, the Sunnah school of thought is a reflection of the Prophet Muhammad’s public actions and private behaviour. Essentially, religion sets boundaries for what is allowed and tolerated. The KSA is overseen by the monarchy, which dominates Saudi politics, with the King and Royal Family effectively running the state. The KSA, therefore, demonstrates a cultural homogeneity that is reflected through a common Arabic language, adherence to the Sunni Hanbali school of Islam, and a common sense of national culture.
1.5.2 The KSA culture
Within the cultural context of the KSA, Islam not only represents a religious ideology but also forms the basis for a social system that defines various aspects of people’s lives. There are, however, divergences in understanding and interpretation within Islam that lead to diversity in compliance with the traditional structures of the Islamic regulatory system and levels of adherence to Islamic ideology. Beling (1980) explains that this diversity within Islamic culture is a result of differences between urban and nomadic characteristics, tribal and non-tribal features, city-dwellers and villagers, and other aspects, such as whether individuals are literate or illiterate, open-minded or conservative.
The KSA has a patriarchal social system, characterised by masculine authority over kinship family groups. This culture affords men control over women, who are considered the ‘inferior gender’, largely due to values attached to the masculine gender as providers and protectors. A lot of emphasis within the social context is placed on the need for individuals to understand and recognise the welfare of others. Saudi social lifestyles are also characterised by specific socially defined ideals for dignity and honour (Beling 1980).
1.5.3 Healthcare in the KSA
Saudi nationals are entitled to public healthcare, which is generally free. The Saudi Arabian Health System is provided by the Ministry of Health centres and hospitals, in conjunction with the King Faisal Specialist Hospital and Research Centre (KFSH&RC), universities, and portions of the military (MOH 2006). Relatively low numbers of Saudis are part of the Saudi Arabian healthcare workforce, which is instead heavily dependent upon workers from other countries, including India, the Philippines, South Africa, the US, and the UK (Al-Dossary et al.2008).
1.5.4 Saudisation
At this point, it is pertinent to mention the concept of ‘Saudisation’. For over a decade, the Saudi government has been attempting to address the imbalance of foreign versus Saudi nationals in the workforce (Ministry of Planning 2002b). This is an issue that is found among a number of the GCC states, such as Qatar and the UAE, where very significant ‘expatriate’ (non-national) populations have developed due to migrant labourers being brought in to fill skills gaps in key employment areas. In comparison with the UAE and Qatar, where the non-national populations are as high as 70-85%, the Saudi population imbalance is relatively moderate at only 27%. It has, however, been identified by the government as requiring a resolution.
A Saudisation programme, which focuses on increasing educational opportunities and thus employment for Saudi nationals, was introduced to reduce and reverse over-reliance on foreign workers and to recapture and reinvest the kingdom’s income (Looney, 2004). The Saudisation process has been slow, and in 2011, Saudi Arabia's Ministry of Labour introduced the Nitaqat (‘zones’) programme as a driving force toward replacing expatriate workers with Saudis in the private sector (Ministry of Labour 2009). The programme categorises companies based on their success at nationalising their workforce, and those companies failing to meet Saudisation targets are penalised (Ministry of Labour 2009). Despite the introduction of the Nitaqat programme, change remains slow. Saudi patients still receive their care within a multi-cultural environment, largely from non-Saudi (and non-Arabic speaking) healthcare workers.
1.6 Healthcare within the KSA
There is a substantial volume of literature that criticises the level of care provided to patients in the KSA, including fluctuations in facilities, insufficient access to cancer management drugs, substantial communication issues, resource challenges, and difficulties in handling necessary organisational restructuring (Almuzaini et al. 1998; Al-Eid and Manalo 2007; Elkum et al. 2007; Brown et al. 2009; Shamieh et al. 2010). Alongside this, healthcare costs in the KSA have been increasing since 1990, and a significant result of this is a shortage of resources and variations in the quality of healthcare provided (Akhtar and Nadrah 2005; Al-Ahmadi and Roland 2005; Walston 2008; WHO 2009).
These issues can partly be explained by the significant socio-economic and infrastructure transformations that the KSA has faced over the last 30-40 years, and the change in its epidemiological profile from infectious diseases and nutritional deficiencies to the ‘age of degenerative and man-made diseases such as cancer and heart and cerebrovascular disease (Younge et al. 1997, p. 309).
1.6.1 The doctor-patient relationship and disclosure
Doctor-patient relationships and disclosures are considered influential factor that impacts patient satisfaction and further patient experience. The central practice in healthcare revolves around the doctor-patient relationship and becomes an imperative component to ensure the delivery of high-quality health care. According to Kelley et al. (2014), the patient must have confidence in the competence of their doctor and the patient needs to feel comfortable enough to confide in their doctor. It is obvious that within the relationship the doctor is recognised as superior to the patient due to his/her extensive knowledge and credentials in the medical field (McKinstry 1990).
Confidentiality is a major factor which influences the doctor-patient relationship as it requires that the health care provider keeps the patient’s personal health information private unless the patient gives their consent to disclose the information. Disclosure of a patient’s medical information without consent leads to a breach of confidentiality which can be tried by law depending on the laws and ethics of various countries.
The doctor-patient relationship in KSA is completely different to the ethically set standards of many Western countries. It is commonly found that many doctors practising in KSA do not follow many of the ethical values that are embraced within a general doctor-patient relationship. This commonly includes a breach in confidentially through casually disclosing patient health information. There are also instances of doctors with KSA's mentality feeling extremely superior to their patient’s causing them to not include patients’ decisions about their health. An in-depth discussion takes place in Chapter 2, Section 2.5.2 which discusses at length literature surrounding the definition of doctor-patient relationships, how the variable influences patient satisfaction, and the doctor-patient relationship experienced in KSA.
1.6.1 Cancer prevalence and care of oncology patients in the KSA
The issue of patient satisfaction in the KSA is particularly pressing in oncology wards, as the cancer rate has been rising in recent years. Even though the top five types of cancer affecting males and females, as reported by the age-standardised incidence rate (ASR), have historically been lower in the KSA compared to the USA, such differences will, according to Ibrahim et al. (2008), be less evident in the future. The incidence of cancers in KSA is likely to increase over the next two to three decades. Reasons for this include an ageing population, the recent adoption of a typically sedentary lifestyle combined with a Western diet, and an increasing number of smokers (Jazieh 2012). Moreover, a recent publication discussing the burden of breast cancer in KSA anticipates that the incidence and mortality of cases are to increase by about 350% and 160%, respectively, over ten years by 2025 (Ibrahim 2008). The reason for such a large increase in these variables may be due to an anticipated prevalence of reproductive factors associated with the increased risk of breast cancer, including early menarche, late childbearing, fewer pregnancies, use of menopausal hormone therapy, as well as increased detection through mammography, as witnessed in developed countries (Parkin and Fernandez 2006; Zahl et al. 2008).
Most significantly, the highest increase in cancer cases in the KSA is predicted for the coming two decades (WHO 2009). Consequently, there is a need for research to examine, inform and make a contribution toward improving the quality of care to meet these anticipated increasing demands. In this regard, the current study addresses patient satisfaction interfaced with the current quality of care received within oncology ward settings in the KSA.
The most recent Saudi Cancer Registry (SCR) reports on cancer prevalence and rates indicate that the total number of reported cases was 13,706 in 2010 (Saudi Cancer Registry 2010). This rate is relatively evenly divided in terms of gender, with 48% of those affected being male (6,579 cases) and 52% being female (7,127 cases). Men were found to have an increased rate (up to 1.5 times the normal rate) of cancer after the age of 64, and the median ages of sufferers were calculated to be 51years for women and 58 years for men. The report also disclosed a geographical division, with Riyadh (central), Tabuk (northwest), Makkah and the Eastern Province having the highest rates, which were measured as 115.00, 92.00, 77.00 and 116.00 (all per 100,000), respectively in 2010 (Saudi Cancer Registry 2010). Further information from the Saudi Cancer Registry’s 2010 report is shown in the figure presented in Appendix 1.
It has also been reported that resources for cancer control in the KSA are inadequate and directed almost exclusively to treatment, with little focus on prevention and screening for early detection (Rastogi et al. 2004). In recognition of the problems posed by cancer, and to alleviate the suffering of people and improve their quality of life in the future, an initiative was launched in 2010 in Riyadh with the stated goal of ‘Improving Cancer Care in the Arab World’ (ICCAW 2010). This high-profile collaboration between the National Guard Health Affairs Oncology Department and the Arab Medical Association Against Cancer also includes the participation of a number of other national and international bodies. The collaboration examined a wide range of themes associated with comprehensive cancer care and control, including the role of service organisations. It was agreed to formulate a strategic planning process for the next ten years, dedicated to implementing improvements to services and planning, and exploring other issues affecting medical reform.
This huge initiative takes a holistic view, examining a range of topics, including funding, detection and screening, access to medication, and human resources development, as well as the establishment of population-based registries across all Arab countries as part of a newly developed National Cancer Control Program to enhance oncology care, generally. By illuminating the doctor-patient and nurse-patient relationship in the KSA, the current study contributes to the understanding of how these relationships operate in the KSA in particular, and Arab countries in general, with their distinct cultural beliefs.
1.6.2 Personal rationale for the study
As a former head nurse within an oncology unit in the KSA, before the current research, I was at the cutting edge of healthcare and dealt daily with a wide range of care being delivered to cancer patients. Through my hands-on experience, I witnessed areas which I believe could be changed to improve the quality of the care that patients receive. In particular, I believe that the circumstances and complexities of each patient should be considered. Such patient-centredness would help remove barriers to top-quality care and allow the patients to become empowered by allowing their opinions, feelings and perspectives to be taken into account.
However, the value of patient-centredness must be recognised before it can be effectively implemented and have a positive impact on healthcare quality. Consequently, there is a need for further research in the field to expand the knowledge base and interpret the relationship between patient experience, patient satisfaction, and quality of care. These personal perspectives and experiences have been a driving force in motivating this research. Moreover, my experiences and knowledge proved invaluable during the conduct of the current study.
1.7 Research methods
A sequential mixed-methods approach was employed to explore factors that impacted patient satisfaction as an indicator of the quality of care, using both quantitative and qualitative methods. To achieve the process of MMR process it was necessary to first conduct a quantitative phase and then a qualitative phase in which a sequential explanatory mixed methods mode was followed.
Decisions about study design were made with care. The use of mixed methods was necessary because, as noted previously, patient satisfaction is a complex construct that can be measured both quantitatively and qualitatively. As Al-Rubaiee (2011) stated, patient satisfaction is ‘psychological’ and thus it is easy to understand but difficult to define; this makes the qualitative approach especially useful. According to Hudak et al. (2000) to assess patient satisfaction, it is recommended to supplement a multidimensional measure that includes global questions through direct measures with open and close-ended questions. Hudak et al. (2000) also suggested combining interview data with various survey questions as they may result in an improved understanding of patient satisfaction.
Therefore, a mixed-methods approach was used as it utilises both quantitative and qualitative methods. Generally, the quantitative approach is commonly used in clinical trials to measure different factors such as pain and disability (Hudak et al., 2000). On the other hand, qualitative data is used as it contributes to policy and practices. Usually, qualitative research includes data collection to describe and explain the meanings people assign to a particular phenomenon (Creswall and Plano-Clark 2011). The purpose of the current study was to explore patient satisfaction within oncology wards using a mixed-method design for this examination. The larger purpose of the study is to contribute to the evidence base for recommendations to be used in enhancing patient satisfaction in oncology ward settings in the KSA, and these two different methods provided wide-ranging data for in-depth analysis in terms of the research aims and questions.
In summary, in the quantitative phase, the participants completed the questionnaire on patient satisfaction to provide data on that variable’s correlations with other variables associated with quality of care, including clinical effectiveness and accessibility. This was then followed, in the qualitative phase, by semi-structured interviews to explore further the quantitative results and to seek patients’ views.
1.8 Outline of thesis
The current study is organised into six chapters.
This introductory Chapter 1 which preceded this section provides an overview of the purpose of this study. The chapter also highlights the reasons for the need of conducting this study. The chapter provides an overview of the aims of the study which will be used later to assess if the study has completed these aims.
Chapter 2 consists of a review of relevant literature related to the aims of the thesis. These include quality of care (including Donabedian’s model), patient satisfaction (including definitions, influences, and approaches to measurement), and KSA-specific studies on patient experience or satisfaction.
Chapter 3 describes the chosen research methodology and methods, and provides the rationale for adopting a sequential mixed-methods approach. This chapter also includes the processes/methods by which the research for the current study was conducted. Chapter 3 provides insights into the justification for the use of the MMR approach to complete the study.
The research findings are presented in the subsequent two chapters: Chapter 4 details the results from the quantitative phase of the study, and Chapter 5 presents the findings from the qualitative phase.
One particular challenge in a mixed-methods approach is to integrate the different strands; this is achieved in the final discussion and conclusions found in Chapter 6, which pulls together and evaluates all of the results, considers the success and limitations of the research, and offers recommendations for further study along with the contributions that the current study makes to the field of patient satisfaction in particular to the KSA healthcare setting. Chapter 6 of the current study also provides insight into the significance of the study along with the various contributions produced to improve patient satisfaction within healthcare delivery in the Saudi Arabian context. The recommendations produced by the study contribute to the improvement of healthcare systems in Saudi Arabia.
Chapter 2 - Literature Review
2.1 Introduction
This review begins with a description of the methodology used in the literature search strategy, and the narrative synthesis method that is used to combine or pool the results of research studies with a range of different research designs (Coughlan et al. 2013). Then, the chapter discusses the literature on (a) quality of care and the use of the Donabedian model to define it; (b) patient satisfaction, a vital aspect of patient experience, which is a concept based on the attitudes of a patient towards their care and evaluation of the quality of care and (c) the assessment of patient satisfaction and quality of care in the KSA based on the patient experience, its factors of influence, and various means of measuring patient satisfaction in KSA along with its issues.
In the third section, which follows the discussion of the quality of care and patient satisfaction, a thorough appraisal is made of the selected literature regarding patient satisfaction in oncology settings in the KSA. A careful assessment of the most robust evidence and a detailed exploration of important and relevant themes emerging from the studies are then offered. The review concludes by identifying the limitations of existing patient satisfaction studies. These limitations are subsequently used to help formulate the research question adopted for the current study, and help to articulate the research question and the research design.
2.2 Methodology for literature review
2.2.1 Narrative synthesis
This chapter provides a narrative synthesis of existing relevant literature in the KSA and beyond, focusing primarily on publications from the last three decades, as there is little published material on the topic from before 1980. The method of narrative synthesis has been chosen from among the different methods for conducting a literature review identified by Popay et al. (2006) because it relies primarily on words and text to explain, interpret, and summarise the synthesis of findings from multiple studies which inform the research question. Narrative synthesis is a particularly useful method for facilitating evidence-informed policy development internationally (Snilstveit et al. 2012). Popay et al. (2006 p. 5) define narrative synthesis as an:
Approach to the systematic review and synthesis of findings from multiple studies that rely primarily on the use of words and text to summarize and explain – to ‘tell the story – of the findings of multiple studies.
The narrative approach to the synthesis of research evidence involves critical appraisal of large bodies of evidence, which can employ different research designs, including qualitative and/or quantitative, or a combination of both - mixed methods. The narrative approach is particularly relevant to synthesise diverse evidence from a range of study designs, as is the case here. It is noteworthy that, unlike the commonly used specialist synthesis methods, narrative synthesis has not been well developed. For example, one particular weakness of narrative synthesis mentioned in the literature is the lack of transparency (Dixon-Woods et al. 2005) and the lack of clarity on methods and guidance on how to conduct such a synthesis (Mays et al. 2005).
However, within the past decade, extensive work by Popay et al. (2006) has culminated in published guidance on the conduct of narrative synthesis. This guidance shows researchers precisely how to conduct narrative synthesis systematically and transparently by focusing on the synthesis of evidence, the effectiveness of interventions, and factors determining the implementation of interventions. This guidance has been tested by other researchers and found to be robust and transparent (Arai et al. 2007; Rodgers et al. 2009). It has, however, been emphasised that researchers should ensure their narrative synthesis is aimed at producing a reflective account, rather than simply providing a summary of research findings (Rodgers et al.2009).
Applying this guidance to the current research ensured effective implementation of the technique. Specific tools to assist in the synthesis were adopted, and the narrative synthesis was followed. First, the approach involved setting out the adopted search strategy and describing the reasons for including particular articles. Second, theories were developed and a preliminary synthesis of the most robust research evidence was performed. This was then followed by an evaluation and a reflective account of those articles selected for inclusion. Finally, conclusions and recommendations are offered. The process is shown in the flow diagram in Figure 1.
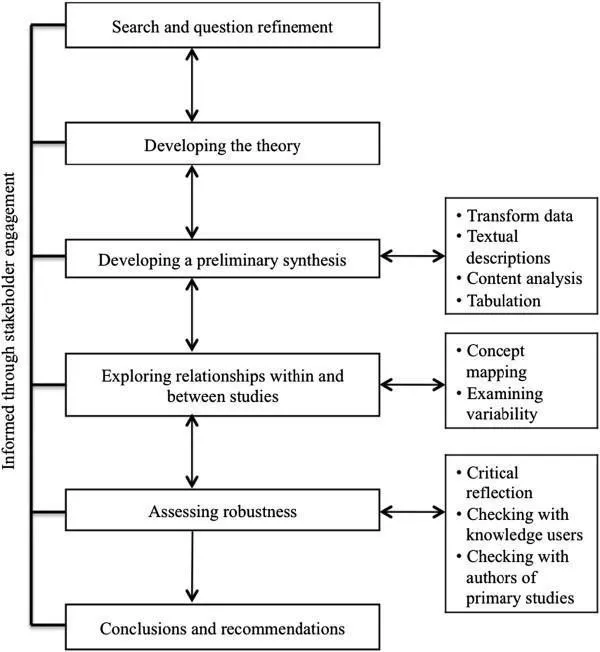
Figure 1 - Integrative narrative synthesis process (adapted from Popay et al. 2006)
2.2.2 Literature search strategy
The selection criteria used for this review were applied in two stages. The initial selection of studies was followed by a final selection of the studies after an appraisal of quality. As previously mentioned, the literature search was kept within the date range of 1980-2014, as there is little published material on the topic before 1980. This also covers the period during which there was a substantial socio-economic change in the KSA, as discussed previously.
Multiple databases were searched, including Science Direct; CINAHL (Cumulative Index to Nursing and Allied Health Literature); Web of Knowledge (multiple databases, including Medline); and Google Scholar. Combinations of search terms were used through the Boolean operator, including: ‘patient satisfaction AND quality of care, ‘patient satisfaction AND Saudi’, ‘Saudi patient satisfaction’ AND ‘quality of care, Saudi Cancer patient satisfaction AND quality care’, ‘quality health care AND Saudi’, ‘Doctor Communication AND Saudi AND cancer care’, ‘Communication AND Saudi Cancer care’. This search strategy facilitated the capture of all articles about quality care issues in health care, both globally and in the KSA, with a specific focus on oncology patients. In addition to this database search, other documents and reports were accessed via the Saudi Ministry of Health, and Saudi Cancer Registry websites. A total of 93 papers were retrieved following this search (see Appendix 2 for the search and screening process).
2.2.3 Inclusion and exclusion of all search outcomes
Following the initial search, the next stage of the selection process was to narrow down the articles by reading through the abstracts and removing those not directly related to the current study. The inclusion and exclusion criteria used for this selection are shown in Appendix 3. After this secondary review was complete, a total of 69 articles were selected for a full review. The importance and value of hand searching during systematic reviews are demonstrated by Armstrong et al. (2005) who use the same criteria as described for the current study. Therefore, a further 21 additional articles were selected by hand searching the citations from the initially selected articles and identifying those articles considered of relevance. These were subsequently narrowed down to nine. Accordingly, a total of 78 papers were ultimately collated and subjected to a quality appraisal.
2.2.4 Quality appraisal
To determine the quality of these extracted papers, all of the 78 identified primary studies were further subjected to rigorous quality appraisal using the method devised by Dixon-Woods et al. (2005). This approach does not exclude weaker studies but gauges the overall quality of both quantitative and qualitative papers to be graded together using the following five criteria: (1) aims and objectives, (2) research design, (3) methodology, (4) findings, and (5) interpretations and conclusions (see Appendix 4). One point is given for each of these aspects, and a research paper’s quality is judged in terms of the total score obtained out of five. Of the 78 papers, those obtaining the highest quality appraisal rating were included in the final review. These papers were scored in the following way: 3, if they omitted a robust explanation of the methods used such as the sampling strategy or the instrument definition; 4 if only a clear interpretation of the results was missing; and 5, if they addressed study aims, methods and findings. As a consequence of this screening, a total of 58 papers were selected for use in this review.
2.3 Overview of studies
This section presents an overview of the studies reviewed. The details of the 58 papers that were selected and critically reviewed can be found in Appendix 5. Appendix 5 includes a summary of study aims, sample population, methods, key findings and limitations of the studies for each paper. A preliminary synthesis helped develop theories regarding patient satisfaction; further critical review then allowed exploration of relationships within and between studies. This iterative process identified a number of common themes and allowed for the categorisation of several identified variations. The rest of this chapter presents the narrative synthesis of the research on the quality of care, patient satisfaction, and healthcare in the KSA.
2.4 Quality of Care: Definition and Measurement
Quality of care is an increasingly important concept in health care. However, it has proved a very difficult concept to measure and quantify given its highly subjective nature (Cleary 1998; Campbell et al.2000; Ladhari 2009; Beattie et al. 2014). Therefore there is a need for a working definition that can capture the multidimensional nature and reflect the differing perceptions of what comprises quality of care. The Institute of Medicine IOM (2001) define quality as ‘the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge (IOM 2001, p.65). This definition suggests that if patients can access the services they need and if the services provided are useful then quality is guaranteed. Therefore, this working definition is adopted in the current study.
The traditional method of measuring the quality of health care was assessing if the care or treatment being provided had achieved its goal, for example, was the illness was cured, did the patient recovered (Payne et al. 2001). Today a more holistic approach is taken to the issue of quality of care. Quality of care is ultimately how patients reflect upon their experiences in a health setting and if they positively construct them. Therefore the quality of care is ultimately determined by the patient and this is crucial to a patient-centred approach (IOM 2001). Quality of care usually involves more than successfully treating a patient and is related to the overall experience of a patient (Tsianakas et al.2012; Manary et al 2013; Beattie et al. 2015). An important theme that emerged in the literature review was the wide range of components of care and the differing extents to which they have received attention. This raises the issue of the identity of the indicators we need to consider as essentially linked to the measurement of quality to assess patient satisfaction.
The most frequently identified dimensions of quality in literature are safety, effectiveness, efficiency, equity, patient-centeredness and timeliness (IOM 2001; WHO 2006; Copnell et al.2009; Beattie et al. 2015) all of which will be reviewed in the current study’s literature review section. . Campbell et al. argue the vital importance of effectiveness as a major criterion for measuring the quality of care as effectiveness is related to all clinical aspects of health care delivery. However, the focus of the current study is to assess patient satisfaction through understanding patient experience in oncology wards in the KSA healthcare settings. For this purpose, all six quality dimensions identified in the literature will be assessed.
2.4.1 Donabedian model
The Donabedian model (1980) provides a framework to understand the quality of care in a healthcare setting. It does not claim to offer how an organisation can improve the quality of care, or even present a definition of what quality of care is, but rather should be seen as a way of helping to evaluate it. The Donabadian model offers a way of analysing a health care environment or a treatment method to determine what can be done to understand the level of quality of care for patients. Information on patients’ satisfaction with the quality of care can be assessed with the help of information captured under three domains (1) process, (2) structure, and (3) outcome which for the current study are used in combination with IOM’s (2001) six dimensions of quality which includes safety, effectiveness, equity, patient-centeredness, efficiency, and timeliness. The information captured under these domains is all specific to aspects of care including quality found throughout the healthcare system. The structure is the context and environment in which the care is provided. This can include the buildings, equipment and staff. Process refers to the various actions and initiatives taken in the treatment of a patient and includes all the actions involved in the care of a patient from diagnosis to aftercare. It includes clinical and interpersonal aspects of care during the delivery of medical treatment or intervention. Outcome refers to the series of consequences and effects of the treatment on a patient. This is possibly the most important of all the concepts in the Donabedian Model. It is ultimately the main criteria for a patient’s level of satisfaction with the care received.
The Donabedian Model does not try to measure the quality of care; rather it provides a theoretical framework that allows professionals to examine the factors involved in the quality of care for patients. There is a strong relationship between all three domains as suggested by Donabedian (1980) and all need to be explored together (Khmais and Njau 2014, p. 6). For example, the Donabedian Model was used as a basis to construct reliable findings on patients’ satisfaction in an outpatient setting in Dar Es Salem Tanzania (Khamis and Njau, 2014). The model has been widely used as the basis for identifying quality in international healthcare settings (Tarlov et al. 1989; Irvine and Donaldson, 1993; Campbell et al. 2000; Kringos et al. 2010). The model has been used to generate data and insights into patients’ quality of care and provides concepts useful in identifying factors that influence patients’ satisfaction and has been useful in the current research
2.4.2 Influence of Donabedian’s model
Debates and findings in the literature regarding the quality of care demonstrate the widespread influence of the Donabedian model and appear to centre upon organisations’ service structures and processes, plus doctors’ and nurses’ skills and availability (Chassin and Gavin 1998; Copnell et al. 2009). In a study on quality of care in hospitals by Copnell et al. (2009), indicators were first classified based on aspects of care provision (structure, process, and outcome), then according to the dimensions of quality (safety, effectiveness, equity, patient-centeredness, efficiency, and timeliness), followed by the domain of application using the Donebedian’s model, including hospital-wide surgical and non-surgical clinics. The study of Copnell et al. (2009) found that while there were a large number of available indicators, there were instances where they were not applicable and inadequately measured the quality of care, and further studies were needed to determine which of the existing indicators are pertinent.
Research suggests that the structural aspects of healthcare have implications for patient satisfaction. Structure of care refers to ‘the organizational factors that define the health system under which care is provided (Campbell et al. 2000 pp. 1612). A key domain of a healthcare delivery system is how it is structured to involve service organisations or access to services in the healthcare facility (Donabedian 1980; Davies and Crombie 1995; Campbell et al. 2000; Sizmur and Redding 2009). This includes the ease and rate of the movement of patients from one facility to another, the availability of services, such as screening and testing, the effectiveness and organisation of the schedule that the patients have to follow, and the overall experience of the patients during their time in health care. Patients’ experiences of access to services, which include service organisations and structures, can significantly contribute to patient satisfaction, which is one of the key indicators of quality of care. Hence, assessing access to services represents a further dimension needed to meet the aims of the current study.
Research further suggests that the processes by which healthcare is delivered are related to patient satisfaction. According to Campbell et al. (2000), Donbedian’s process of care ‘involves interactions between users and the health care structure; in essence, what is done to or with users’ (pp.1612). Of fundamental importance to processes of care is clinical effectiveness, an important criterion for patient satisfaction (Schuster et al. 2005; Campbell et al. 2009). Clinical effectiveness is the delivery of suitable patient care suitably by health professionals with the best outcome possible for the patient and their wellbeing (Doyle et al, 2013).
Studies by Cleary and Edjman-Levitan (1997), Chassin and Gavin (1998), and Campbell et al. (2000) describe a plethora of different quality indicators with little standardisation. A study, undertaken by Bredart et al. (2007), using the EORTC INPATSAT32 questionnaire, found that the most relevant indicators of quality were the interpersonal skills and availability of nurses and doctors, and information provision. The EORTC INPATSAT32 tool is cross-culturally validated and is therefore found to be capable of judging the satisfaction level of patients from different cultures. The difficulty in measuring the quality of care was confirmed by some studies to be due to a lack of a standardised definition of what comprises quality and how best it can be measured (Mainz 2003; Groene et al. 2008). Mainz (2003) differentiated quality based purely on structure (number of specialist doctors available, access to equipment and tests, access to specific units, etc.), process (protocols and procedures that were used in treatment and care), and outcome (mortality, health status, satisfaction and patient quality of life). From the consensus in the literature, it is now clear that when considering the patients’ perspectives of their care, a range of influencing factors, including social-political, social-cultural, and socio-demographic, must be considered. Given the difficulty of defining and measuring the quality of care, it stands to reason that it would also be difficult to measure patient satisfaction, the construct at the heart of the current study. However, the indicators discussed above in the Donabadian model allow for parameters to be established to allow the issue of patient satisfaction to be explored.
2.5 Patient satisfaction
This section discusses the literature on patient satisfaction, including (1) the varying definitions of the construct of patient satisfaction, together with (2) the wide array of factors that have been shown to influence it, and (3) the various approaches that can be used to attempt to measure it.
2.5.1 Definitions
The concept of patient satisfaction has evolved over the years as different definitions have been applied to the concept. Linder-Pelz (1982) defined patient satisfaction as an evaluation of distinct health care dimensions. Pascoe (1983, p. 189), on the other hand, defined it as a ‘comparative process involving both cognitive evaluations of care and an affective response that may include both structure process and outcomes of services. Keith (1998, p. 1122), defined patient satisfaction ‘as a complicated multidimensional concept whose measurement and application are anything but simple. A more recent definition by Al-Rubaiee (2011) refers to it as a psychological notion that is easily understood but difficult to define. Patient satisfaction is considered an imperative and generally used indicator for measuring the quality of healthcare delivery. Prakash (2010) has argued that patient satisfaction impacts clinical outcomes, patient retention, and medical malpractice claims. Furthermore, it is known to affect the judiciously, efficiently, and patient-centred delivery of quality health care (Prakash 2010). As a proxy, patient satisfaction is considered a very effective indicator used to measure the success of doctors and hospitals. Generally, patient satisfaction is used as a performance indicator commonly measured in self-reporting studies and at times particular kinds of customer satisfaction metrics (Farley et al. 2014). William (1994) and Farley et al. (2014) have countered the effectiveness of patient satisfaction as a useful tool of measurement by arguing that many times self-reporting assessments are unable to measure the extent to which a patient may be content with the healthcare that they are receiving. They argued that metrics implemented may not be valid as patients may be dissatisfied with health which improves their health or satisfied with health care which does not. Various studies have failed to identify the relationship between satisfaction and health care quality including Schneider et al. (2001); Avery et al. (2006); Clarke et al. (2006); Chang et al. (2006); Sack et al, (2011); and Solberg et al (2011);.
These definitions developed through the various literature that has been analysed identify patient satisfaction as a multidimensional concept determined by the individual views of patients asked to complete a questionnaire evaluating the adequacy of care services they have received.
Traditionally, patient satisfaction is largely determined by patients’ evaluation of their experiences, across a range of key variables, especially outcomes. This view of patient satisfaction is often regarded as a flawed concept if it is simply based upon perceptions of quality of care. More recent research on patient satisfaction is now increasingly linked to how they constructed their experiences (Davies et al.2011; Anhang Price et al. 2014). Patient satisfaction is no longer just based upon patients’ ratings of their care but on how they have conceptualised it. That is how they have configured their experiences into a belief or idea that their experiences were positive or negative. This construction involves ‘their multiple satisfactions with various objects and encounters that comprise their care’ (Singh, 1989, p. 177). Patient satisfaction is the conceptualisation of their experiences as good or bad and the extent to which this concept is positive or negative determines their level of satisfaction. Patient satisfaction is distinct from their experiences, although dependent upon those experiences. Patients’ experiences are the encounters with healthcare professionals in a healthcare setting. In other words, it is the sum of all interactions that are shaped by a healthcare organisation’s culture, that influence the patient perceptions throughout the continuum of care (Solberg et al. 2011). Satisfaction is the conceptualisation of the totality of their experiences in a health care setting which is influenced, but not determined, by one experience. Patient satisfaction is defined as the evaluation of the conceptualisation of their experiences and the extent to which it has satisfied their needs and has delivered the expected outcomes (Jekinson et al.2002). This working definition is adopted throughout the thesis.
Central to patient satisfaction are patient expectations. Satisfaction in the clinical setting can be defined simply as the desirable outcome of care, while perceived service quality refers to the process where the consumer (in this case the patient) compares his/her expectations with the service he/she has received, which, in this case, is a subjective measure (Gronroos, 2000). Smith (1992) likewise recognises the subjective nature of patients’ evaluation of care, thus illustrating the complex interrelationship between perceived need, the expectation of care, and the experience of care. Indeed, patients’ expectations of care are known to be influenced by several factors, including patient characteristics, prior experience and characteristics of the situation, as well as environmental factors (Oberst 1984). Expectations predispose a patient to have a positive or a negative experience. Satisfaction levels are related to whether a patient’s expectations are met when they encounter the health care system (Bowling et al. 2013). The extent to which a patient’s expectations have been acted upon or not influences the development of their experience in a healthcare setting which later significantly influences their development of a specific level of satisfaction ( Bowling et al. 2013).
Customer and patient satisfaction constructs are only similar in that they both value the process by which services are delivered. For a patient, service delivery includes medical care as well as provision of comfort, emotional support and education (Kupfer and Bond 2012). Also, there is a suggestion that to satisfy patients continuously, there is a need for physicians to incorporate patient perspectives into the clinical decision-making process. Patient satisfaction can be misinterpreted as there is more to it than a health service provider offering high standards of care and ignoring individuals’ perspectives. Good quality health care by itself does not guarantee that patients evaluate their experiences in a positive light. Findings in the literature recognise the need to differentiate between the two concepts of quality health care and patient satisfaction (Cleary 1998; Haddad et al. 2000). Al-Rubaiee (2011) describes satisfaction as a moving target that must be monitored to understand the content of patient expectations and ensure health care providers respond proactively to enhance the standard of care provided to patients. In other words, patient satisfaction should be supported by abilities and a need for ongoing evaluation of the quality of care to identify opportunities for service or care innovations.
A review of the literature has shown that patient satisfaction is affected by the model of patient-centred care adopted (Brown et al. 1999; Mead and Bower 2000), and evidence has suggested that the underlying notion of what patient-centred care means has implications for patient satisfaction (Michie et al. 2003; McCormack et al. 2011; Kupfer and Bond 2012). However, there is a dearth of literature related to patient-centred care in the KSA. The literature that does exist suggests that the adoption of patient-centred care in the KSA can help bridge the gaps related to information provision resulting from cultural beliefs (Younge et al. 1997; Al-Ahwal 1998; Aljubran 2010).
2.5.2 Influences
Various factors influence patient satisfaction which will be discussed in extensive detail in the following sections. To review, patient satisfaction found in the health care services setting is dependent on factors of healthcare service duration and efficiency of care, the empathy and communication that health care providers give. Evanschitzky et al. (2011) assert that patient satisfaction is seen to be favoured by a good doctor-patient relationship. Mittal et al. (2007) have argued that patients who are well-informed about the process and procedures within a clinical encounter and the amount of time that the processes will take are generally seen to be more satisfied with the service even if they must wait longer. Mittal et al. (2007) also argue that one of the most influencing factors of patient satisfaction is the job satisfaction that is experienced by the healthcare provider.
The research suggests that a variety of different factors influence patients’ perceptions of their experiences in a health care setting, although patient satisfaction is generally difficult to isolate from overall clinical outcomes. This section starts by discussing several cultural and demographic influences more generally and then focuses on specific influences that are found consistently in the patient satisfaction literature: disclosure practices, gender politics, respect for patients’ religious beliefs, the doctor-patient relationship, and the practice of patient-centred care. Afterwards, each of these particular influences is discussed and analysed through the KSA patient satisfaction and experience.
The influences on patient satisfaction are difficult to separate from overall clinical outcomes for several reasons. According to Jackson et al. (2001), the psychological determinants that may lead patients to express themselves as being relatively satisfied or dissatisfied remain largely unknown, a point reiterated in the literature reviewed in this section. To attempt to bring some clarity to these important areas, Jackson et al. (2001) set out to establish which characteristics of patients (and physicians) correlate with expressions of satisfaction, and what the contribution of the many satisfaction variables identified in previous studies may be, and the extent to which the co-relationships remained constant over time. They found that patients over sixty-five years old are more likely to be generally satisfied; however, the most important predictor of satisfaction, according to them, was the meeting of expectations. This supports the findings of Hall and Dornan (1990), who found that higher levels of satisfaction were associated with increased age.
Indeed, considerable research exists indicating older patients tend to be more satisfied with their health care, a phenomenon which is consistent across cultures and nations (Campbell et al. 2001; Crow et al.2002; Jaipaul and Rosenthal, 2003; Sofaer and Firminger, 2005; Moret et al.2007; Quintana et al.2006; Bleich et al. 2009; Rahmqvist and Bara, 2010; Lyratzopoulos et al. 2012). This may arise from older people having lower expectations of the health care system and therefore there is less likelihood of their expectations being unmet. However, some researchers maintain that these findings may be flawed and not a true reflection of reality due to an inherent caution and reluctance of older people to voice their dissatisfaction when questioned about the adequacy of their health services as they are in constant need of them (Bowling, 2002; Bowling et al. 2013). Finally, the findings of this review suggest that there has been little research on the demographics and other patient characteristics as determinants of patient satisfaction in KSA oncology settings; this is an area warranting increased attention.
2.5.2.1 Disclosure practices
An important cultural issue that may impact patient experiences and their reflections on them is disclosure. Research in Japan by Tanaka et al. (1999) found that patients suffering from terminal cancer wanted clarity on their prognosis so that they could make the best use of their time. The study argued that it is a basic human right of an individual to know about his/her prognosis.
Concealing the diagnosis from cancer patients may lead to poor patient compliance, misinformation of treatment options, and side effects, which could hurt the patient’s survival and remaining quality of life. However, even where disclosure occurs, cultural barriers can exist because of a reluctance to accept a terminal prognosis. This puts health care providers in a complex situation, as they are expected to be sensitive toward the patients and their needs as well as continue the care, despite their professional judgment (King et al. 2008). In this regard, it is important to have quality palliative care along with effective coordination between the primary, secondary, and tertiary care services.
2.5.2.2 Doctor-patient relationship
Research further suggests that the doctor-patient relationship is an indicator of patient satisfaction. The encounter between practitioner and patient is valuable for defining patient evaluation of the quality of care and can be seen as fundamental to the doctor-patient relationship (Ong et al. 1995). Although patient-centred communication is at the heart of such interactions, there are different levels and types of communication. These have been separated into three areas by Ong et al. (1995): (1) the creation of good interpersonal relations between the doctor and the patient, (2) the exchange of information, and (3) the making of decisions which are related to the treatment. Ong et al. (1995) found that the extent and type of communication used by the doctor and the responsiveness of the patient will subsequently have a strong impact on the levels of satisfaction derived by the patient from the interaction. Improvements in the doctor-patient relationship will directly influence the quality and levels of patient-centred care, and in the long term, improve patients’ evaluation of their experiences.
In a study of how to improve health through communication, Street et al. (2009) identify seven pathways for doing so: (1) increased access to care, (2) greater patient knowledge and shared understanding, (3) higher quality medical decisions, (4) enhanced therapeutic alliances, (5) increased social support, (6) patient agency and empowerment, and (7) better management of emotions. In another study emphasizing the importance of doctor-patient communication, Kenny et al. (2010) state that good communication is essential if the notion of ‘relationship-centred care is to be encouraged. Their results show some significant differences between what patients perceive as the communication skills of the doctors and the doctors’ perceptions of those skills. The qualitative research by Jagosh et al. (2011) reveals that doctors’ listening to patients is a critical part of the communication process. These results echo the Institute of Medicine’s (2001) claims about the alignment of care to the ‘voice of medicine’ as part of the patient-centred care approach.
These studies demonstrate a clear connection between communication and a successful doctor-patient relationship, and there is some evidence that the more the emotions of patients are satisfied by the doctor through effective and considerate communication, the higher the levels of satisfaction generated. However, there is also evidence that the effectiveness of this relationship appears to depend on the severity and associated psychological condition of the patient (McWilliam et al. 2000; Ong et al. 2000; Street et al. 2009; Jagosh et al. 2011). In other words, whilst a correlation seems to exist between communication and patients’ satisfaction levels, the strength of this correlation remains equivocal and is a subject for further study.
During the past four decades, there has been a transition in the doctor-patient relationship from one in which the decisions of doctors were ‘silently complied with, and any information imparted by the doctor was designed to support his or her opinion of the most suitable course of treatment, to one in which the patient has an expectation of being at the centre of the process and anticipates a greater level of “mutual participation” (Kaba and Sooriakumaran, 2007, p. 57). This shifting relationship reflects not only a change in the socially constructed view of how patients should be empowered but also one which has been encouraged by the ‘social system’. This means that a patient-centred approach has become the predominant model in clinical practice today. However, the KSA is just starting to address the need to improve doctor-patient communication (Aljubran, 2010), and this aspect of research forms an important element of the current study. The next section discusses patient-centred care in greater detail.
2.5.2.3 Patient-centred care
Generally, patients’ development of their experiences based upon their care may involve complex processes and may be influenced by the values and beliefs of each patient, along with other variables such as health status and socio-economic status. A further factor frequently mentioned in the literature on patient satisfaction is patient-centred care (De Silva, 2014). Within the UK, the need for a patient-centred health system is widely accepted, since this approach supports people in making informed decisions about their health and care, hence, facilitating appropriate management of their care (De Silva 2014). The need for patient-centred care is also well-recognised globally (IAPO 2006; WHO 2008), and in 2001, the Institute of Medicine (IOM) highlighted it as a major goal for improving health care in the USA. The IOM report defines patient-centeredness as ‘providing care that is respectful of and representative to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions (IOM 2001, p. 3). Kupfer and Bond (2012, p. 139) describe patient-centred care as ‘improving health literacy through information and education, coordination and integration of care, physical comfort, emotional support, and personalised care, which encompasses the concept of shared decision making. It can be argued that achieving a better experience for a patient and therefore higher patient satisfaction levels involves good patient-centred care (Krupat et al. 2001; McCormack 2003).
The ascent of patient-centred care in recent years has been driven by the recognition that care can often be more effective when it is tailored to specific patients’ needs (Gill, 2013). Patient-centred care in the literature is very much focused on the individual, the delivery of whole person-care and communication. This form of care encourages the participation of the patient and their family in the decision-making process about treatment. Although researchers disagree on what exactly constitutes patient-centred care, and its influence on patient satisfaction has not been firmly established, ample evidence does suggest that patient-centeredness leads to patients reflecting upon their experiences in a health care setting in a positive way. Patient-centred care is still fairly new in the Saudi healthcare delivery system due to societal norms that influence doctors' and nurses' perceptions.
Indeed, the literature reveals the existence of several definitions for patient-centred care and, largely as a result of this; there is a range of approaches available for measuring patient-centred care. Most take a holistic view or measure specific subcomponents such as shared decision-making or communication (De Silva 2014).
2.5.3 Factors influencing patient satisfaction in KSA studies
Throughout the literature, strong patient care has been established as a strong indicator of PCC but it is very little to no literature available of evidence of PCC in KSA. In the KSA, other influences have also been identified, such as culture and language differences between KSA nationals and health care practitioners, and these have been found to affect the perceived quality of care patients receive. This is largely influenced by the fact that the nursing workforce in the KSA relies mainly on expatriates who are recruited from different countries such as India, the Philippines, South Africa, North America, the United Kingdom, Australia and the Middle East countries (Luna 1998; Tumulty 2001; Aboulenien 2002). One study showed that the language and cultural differences of the expatriate nurses may cause Saudi patients to encounter barriers to communication during health care (Al-Dossary 2008). Thus, the challenge for the KSA is to increase the proportion of Saudi nurses in the workforce to deliver culturally sensitive care, further facilitated by all nurses having a command of the Arabic language used by Saudi patients (Al-Dossary 2008). This would enhance the experience of patients and allow them to construct their experiences positively. Notably, however, an earlier study argued that language differences between patients and nurses do not impact the satisfaction level of the patient (Ibrahim et al. 2002). These findings call for more research into KSA patient satisfaction, specifically in terms of language and cultural differences between patients and nursing staff.
Other factors highlighted as potentially affecting patients’ perception of their experiences and the subsequent level of their satisfaction with care in the KSA are political-social, age, or educational issues. Patients who are better educated but have poor health are more dissatisfied than those who were less educated and in better health ( (Alborie and Sheikh Damanhouri 2013). Also, older patients tend to be more satisfied with the service quality than those in their twenties ( Alsakkak et al.2008 ). This may be related to the previously mentioned transformation in the economic climate in the KSA. Older people may be more accustomed historically to living in austere conditions and therefore have lower expectations of the healthcare system and are appreciative of whatever care they receive (Bowling et al. 2013). Rahmqvist and Bara () likewise identified patient characteristics related to patient evaluations of their experiences in a health care setting, namely age, education and health status.
A systematic review of the available literature conducted by Williamson and Harrison (2010) confirms that culture plays a role in how patients experience health care. Failure to determine the cultural needs of individuals receiving care contributes to dissatisfaction with health care practices. Williamson and Harrison’s (2010) study can be extrapolated to other countries where there are cultural differences between healthcare providers and healthcare receivers. In the KSA, there is a cultural belief related to the Islamic faith that patients who have terminal illnesses cope best with their illness at home surrounded by family members and friends (Younge et al. 1997). This may act as a barrier to proper health care provision due to communication issues that may arise in such a home-based treatment. For example, whilst doctors and nurses are welcomed into Saudi homes, there may also be a need for drivers, and possibly translators, to accompany them, especially when the patients are women, due to cultural prohibitions related to gender and social interaction (Dein and Stygall 1997; Al-Amri 2010). Moreover, since a large proportion of the nursing workforce is expatriate, while the health care receivers are largely Saudi nationals, there is a potential for language and cultural differences, leading to misunderstanding and unsatisfactory encounters between patients and health professionals (Al-Dossary 2008). In contrast, another study (Arora 2003) argued that the language differences between patients and doctors and nurses do not impact patients’ reflections on their experiences. The study noted above by Ibrahim et al. (2002) found that the patients were satisfied with the doctors’ skills and their interpersonal behaviour, even in cases where there were language differences between them. These contrasting findings suggest that more research is needed to determine the effect of and accurately identify communication barriers (between patients, doctors and nurses) on patient satisfaction. Indeed, a better overall understanding of the causes of the positive or negative views by patients on their experience is very much needed.
2.5.3.1 Disclosure practices
In the KSA, patients are often not given the privilege of being treated as independent individuals but are approached as extensions of the family (Aljubran 2010). Al-Ahwal’s (1998) study in the KSA evaluated the awareness of cancer patients of their diagnosis and prognosis from the perspective of a small population of doctors, patients and lay people. The study uncovered a low level of awareness about cancer patients’ prognosis, despite a desire that they are made fully aware of their conditions and be treated as autonomous individuals. The doctors largely conceded that they preferred to tell the patients the truth regarding their diagnosis and prognosis but in practice, this is not the method that they used which has been discussed within the section on the doctor-patient relationship in Saudi Arabia. Indeed, it is increasingly being recognised that for KSA doctors to provide suitable treatments for their patients, disclosure and effective communication are important issues (Aljubran, 2010; Younge et al.1997). Thus, it is evident that information exchange between practitioners and patients tends to be very low, due largely to poor patient participation in decision-making and/or a lack of patient interaction with doctors or nurses (Elzubier 2002; Al-Amri 2010). As a result, patients may not have full knowledge of their condition, even though they are the ones receiving the care and should be perceived as the key participants in the process.
The KSA health care system is gradually recognising the importance of sharing health care information with patients. There is a new trend in the KSA health system toward encouraging oncology medical staff to keep patients well-informed about their health status. Conceivably, this may enhance patient satisfaction within the KSA (Mobeireek et al. 2008; Aljubran, 2010). As alluded to previously, it is important to recognise how poorly informed patients could create bias in the results and adversely affect the quality of surveys on patient satisfaction.
2.5.3.2 Gender politics
One social issue that hinders the quality of care in the KSA is the cultural background relating to women, who still require permission to seek health care from a male guardian, and cannot freely communicate their needs to health care professionals, especially regarding reproductive health. This can lead to restrictions on access to health care (Walker 2009). Intervention by male relatives can mean that health care professionals cannot properly investigate the illness of the women (McBride 2008). One of the drawbacks that are faced in allotting women's healthcare services in KSA is that many women are unaware of their rights and knowledge of healthcare. For example, many women in KSA are not aware of their right to consent for their medical treatment in addition to doctors also not be aware of this legal right or they deny women these rights out of fear of encountering issues with their male guardians (Al-Amoudi 2012).
Gender inequality within the Saudi context of social stigma hurts women’s healthcare. The distribution of power and resources in Saudi society places a higher preference on men than on women which causes issues in public health policy and practice leading to a decrease in patient satisfaction, mainly among female patients. According to Mobaraki and Soderfeldt (2007), the World Health Organisation has stated that gender inequality is not only a threat to economic development but also to population health, especially for that future generations. The traditional Arab family and society as a whole have a tremendous effect on women’s health in a multitude of ways. Women in KSA are known to have a high prevalence of obesity which is attributed to social restrictions that prevent women from participating in exercise activities in schools or in public although the government does not forbid the female practice of sport in public or segregated private places. Other inequalities include the restriction of women from being admitted into a hospital without their male guardian and not being allowed to give their consent for invasive medical procedures.
For example, McBride (2008) and Elkum et al. (2007) both highlight serious issues relating to breast cancer in the KSA, namely, the cultural stigma associated with the disease, and a lack of empirical research on the protocols or techniques involved in its diagnosis and treatment. Breast cancer is the most common type of cancer among Saudi women, yet there is an exceptionally high proportion of young women not being diagnosed (Elkum et al. 2007; Ibrahim et al. 2008). This is largely due to the inherent barriers to screening associated with cultural issues and leads to problems with obtaining accurate and early detection. This, in turn, has negative ramifications on prognosis (Elkum et al. 2007; Ibrahim et al. 2008) and by extension, on quality of care, which can impact patient satisfaction, which is highly dependent upon meeting expectations. However, studies such as Al-Sakkak et al. (2008), Ibrahim et al. (2008), and Mobaraki and Soderfeldt (2007) have shown that women regardless of the type of treatment allotted to them are more satisfied with their quality of care. According to Al-Sakkak et al. (2008), this is because less educated people tend to be more satisfied with healthcare providers while high patient educational levels resulted in a lower level of satisfaction with the quality of healthcare provided to them.
2.5.3.3 Respect for religious beliefs
Almuzaini et al. (1998) note that since the KSA is an Islamic nation Islam is very influential in healthcare. The provision of religious or spiritual care is often offered in the KSA as a relief mechanism for patients suffering from terminal illnesses (Dein and Stygall 1997). This may be either as an alternative to or alongside palliative medical care. Indeed, Boyles and Nordhaugen (1989) suggest that health care activities are at variance with the religious and cultural norms of the nation, when one considers that under the pervasive influence of Islam, there is widespread acceptance that one must die, and the suffering associated with death is regarded as the show of one’s faith in religion and God. This sentiment is said to help patients cope with cancer better than in any other country in the world (Ezzat et al. 1995; Young et al. 1997; Al-Shahri 2002).
Many doctors and nurses are influenced by western models of care, which are largely secular and strive to provide the best service with a detachment from any religious reasoning of their patients. Clearly, given the issues previously discussed, it could be problematic if doctors lack empathy for such socio-cultural factors during their discussions, prognosis, and treatment of the disease with Saudi patients. This could conceivably create distrust in the health care service and may result in patients negatively building their experiences.
2.5.3.4 Doctor-patient relationship
KSA faces a serious issue in the healthcare system with the poor doctor-patient relationships which as a result is having a strong impact on patient experience particularly patient satisfaction (Elzubair 2002). Patient satisfaction depends a great deal on a doctor-patient relationship as asserted by Weber et al. (2014) who assessed that satisfied patients will follow the medical instructions given, return for follow-up care, and are seen to maintain a longer-term professional relationship with their healthcare provider. However, it is also evident that doctor-patient relationships that are seen as poor result in just the opposite and are just as unsatisfying to doctors (Vermeire et al. 2001; Al-Sakkak et al. 2008; Stravropoulo 2010). Patient satisfaction has become a key issue in healthcare systems within Saudi Arabia and other Arabian Gulf health systems. In the setting of the KSA, practitioner-patient interactions are mostly characterised by the doctor having authority over the patient (Younge et al. 1997; Elzubier 2002). In the KSA, doctors’ attitudes and behaviour have historically been influenced by their own culture (Aljubran 2010). In particular, patients are often viewed as fragile and extremely vulnerable, rather than as individuals with their strengths and capacities to cope with their disease (Younge et al. 1997). Doctors can fail to maintain what in Western contexts would be considered issues of privacy about the patient’s conditions, and disclose ailments to their relatives without the knowledge of the patient (Younge et al.1997; Al-Amri 2010). At the heart of this is the relationship between disclosure and patient autonomy, which historically have been considered quite differently in the KSA. Instead, traditional cultural assumptions have dictated that physicians provide information about serious illnesses, such as cancer, to the family of patients first. The patient is then subsequently informed, but only if the family approve of doing so (Mobeireek et al. 1996; Al-Amri 2010). Thus, the next of kin has access to information regardless of the patient’s knowledge about his or her health situation (Al-Amri 2010). This not only affects the practitioner-patient relationship but also means that the views of patients reported in previously published research surveys found in literature need to be treated with some caution, since patients may lack key information about their care. Therefore, findings from previously published literature on patient satisfaction within the KSA context may be affected by bias and lack of representation among the patient populations that take an active role in medical decisions and their care.
There is certainly broad agreement in the literature worldwide that patient autonomy is an important aspect of quality patient care (McCormack 1992; Gaston and Mitchell 2005). Nevertheless, this model of disclosure and patient autonomy has not historically been practised in the KSA. A decade ago, research by Mobeireek et al. (1996) suggested that the KSA had a long way to go to get to a position where patients, as the actual recipients of fully informed care, are actively involved in decision-making about their care. More recently, Mobeireek et al. (2008) demonstrated an increased recognition of patient autonomy amongst physicians. Weber et al. (2014) suggest that the key factor for these changes is linked to the increase of personal wealth in KSA which is the driving force for higher quality expected from patients including increased attention to a doctor-patient component to ensure patient satisfaction in providing quality care. Similarly, research conducted by Aljubran (2010) and referring to the rapidly changing KSA society has indicated that patients are expecting greater autonomy and are now increasingly demanding that they have full disclosure about their diagnosis and prognosis. This is a major cultural shift, leading to a growing need for patients to be treated holistically and as individuals, and to take their perceptions of satisfaction with their care into account. For example, there is evidence that patients with breast cancer generally prefer to be fully informed regarding the status of their cancer, and to be involved to some degree in decision-making regarding their treatment (Elkum et al; Nichols et al. 2013; Sait et al. 2014). Several studies have proposed that the application of such patient-centred care would help eradicate the undesirable, yet common practice of preventing patients from accessing their medical information (Younge et al.1997; Al-Ahwal 1998; Elzubair 2002; Aljubran 2010). Patient autonomy and disclosure in KSA patients represent only two of the potentially influential aspects relating to patient satisfaction.
Patient satisfaction within the KSA will be affected by how changes in the doctor-patient relationship are managed, especially with changing patient demographics. Cultural and communication difficulties may also contribute significantly to how this relationship is understood, both by patients and by medical staff.
2.5.2..5 Patient-centred care
As presented before, there are very little to no studies that undertake the analysis of patient-centred care in KSA. Therefore, other non-KSA studies were used to contextualise the meaning and rationale of patient-centred care, regardless of which hospital setting it is taken in KSA or otherwise. Therefore, based on a thorough analysis of the literature, various dimensions of patient-centred care were analysed which can be used to help the KSA in implementing PCC based on international standards.
The systematic review conducted by Mead and Bower (2000) identified five conceptual dimensions of patient-centeredness: (1) bio-psychosocial, (2) patient-as-person, (3) sharing power and responsibility, (4) therapeutic alliance, and (5) doctor-as-person (Mead and Bower 2000, p. 1087). They also identified other influential variables such as individual characteristics and consultation processes, suggesting that wider and more complex dimensions may be required before any firm conceptual basis of patient-centeredness can be established. A study of this nature has yet to be performed in the KSA. However, Al-Mutairi and Moussa (2014) have observed that medical staff in KSA are unwilling to understand patients; problems. Many are also not aware of the patient's bill of rights which includes the right of being fully informed of their diagnosis and treatment plan which is a key aspect of patient-centred care (Al-Mutairi and Moussa 2014).
Patient-centeredness has been suggested to positively influence physical and psychological outcomes, however, Michie et al. (2003) argue that the evidence is inconsistent. They reviewed the effects on the outcome of chronic illness of two concepts in health care communication: one in which the health professional took the perspectives of the patients, and the other where the aim was to ‘activate’ the patient by ensuring they took an active role in their health care. It was discovered that in studies where the aim was to activate the patients, the results were more consistently associated with good physical health outcomes (Michie et al. 2003, p. 197). Unfortunately, the application of an ‘activation of patient’ approach may be limited within the KSA due to the cultural norms described above, including issues of disclosure, lack of confidentiality of patient's health status, and poor patient autonomy (Younge et al. 1997; Walker 2009; Aljubran 2010). The proposal of Michie et al. (2003) to activate the patient for improved outcomes would support the need for better communication and a change in the policy on patient information provision and disclosure in the KSA. This would concurrently enhance patients’ understanding of their treatment and allow them to make informed decisions regarding their treatment.
Holmstrom and Roing (2010) suggest that because patient-centred approaches seem to be understood in different ways by different groups within the health care profession, a common language should be created to define the contextual and conceptual meanings of patient-centeredness. They were able to differentiate between the terms patient-centred and patient empowerment but concluded that while the concepts are complementary, patient empowerment has a wider aim, which may place more responsibility on health care professionals. On the other hand, patient-centeredness can be seen as the starting point from which patient empowerment can grow. Unfortunately, patients in the KSA generally have little provision for empowerment, given the entrenched cultural and patriarchal norms which are contrary to a patient-centred-care approach (Young et al 1997; Al-Amri 2010).
McCormack et al. (2011) researched an attempt made by an institution in the United States to promote the use of patient-centred care for oncology patients and point out that no comprehensive measure of such care exists. They imply that research on patient satisfaction fails to focus on certain factors, for instance, how patient satisfaction relates to the patient evaluation of care expectations. There is no general model that can account for how patients construct the concept of satisfaction, and to address this issue, McCormack et al. (2011) conducted a comprehensive review of the existing literature and undertook interviews with selected patients. The research identified six core concepts which are prevalent in the notion of patient-centred care: (1) exchanging information, (2) fostering healing relationships through focus on affective care, (3) recognising and responding to emotions, (4) managing uncertainty, (5) making decisions, and (6) enabling patient self-management (McCormack et al. 2011).
Similarly, Mead and Bower (2000) emphasise the fact that delivery of high-quality health care is contingent upon the use of a patient-centred approach. However, the generalizability of their findings is questionable, warranting further research to test this notion in wider settings. Notably, patient-centred care leading to enhanced patient satisfaction may be adversely influenced by specific socio-cultural contexts. For example, as mentioned previously, in the KSA, patient-centred care does not fit the socio-cultural norm in which doctors are seen as figures of great authority (Mobeeriek et al. 1996; Younge et al. 1997; Elzubier 2002) and attempts to introduce this model may first necessitate a change in the cultural context to support patient satisfaction.
Some studies indicate that patient-centredness has a definite link to patient satisfaction. Studies by Griffin et al. (2004), Bredart et al. (2007), and Rao et al. (2007) which looked at the effectiveness of different approaches aimed at improving doctor-patient communication, demonstrated evidence of a significant relationship between overall health outcomes and their experience of care and patient satisfaction. Fielding (2009) argued that the perception of patient satisfaction and the adoption of a patient-centred approach was important since patients are the end-users of health care services. The importance of taking a patient-centred approach that recognizes the importance of patient satisfaction is assuming an increasingly prominent role in health care systems worldwide, with the patients’ perspectives being increasingly considered an essential criterion for judging the quality of care (IOM 2001; Mallinger et al. 2005; Wolf et al.2008; Arraras et al. 2009).
Whilst there is evidence that patient satisfaction has a strong connection with the doctor-patient relationship, and with the level of positive communication within this relationship (Arrora 2003; Epstein et al. 2005), the connection with patient-centeredness remains ambiguous (Kupfer and Bond 2012; McCormack 2011), although there appears to be some interrelatedness between the two concepts (Jagosh et al. 2011; Bret 2012). Brett and McCullough (2012) argue that patient satisfaction and patient-centred care are not automatically related. The localisation of the concept of patient satisfaction, and hence, the localisation of the concept of patient-centred care, means that patient satisfaction would be differently constructed in different locations. As a result, patient-centred care within the context of the KSA may demonstrate variations from the practice of other countries. For example, the construct of optimised, patient-centred communication may differ between cultures.
Kaba and Sooriakumaran (2007) demonstrate that many physicians do not feel an obligation to meet the demands of a patient-centred care approach. Indeed, the concept of personalised care, which assumes that patients are empowered and work together with physicians in determining their care provision and therapeutic options, is rarely seen in the KSA (Elzubier 2002; Walker 2009; Aljubran 2010). Interestingly, it has been suggested that some evidence of high levels of satisfaction may distort the picture, as some physicians may over-order diagnostic tests and prescribe medications simply to satisfy the emotional needs of patients which is related to their expectations, even though they would not serve to improve patients’ physical conditions (Kupfer and Bond 2012).
In summary, it can be noted that there is diversity when it comes to clearly defining the term patient-centred care. However, based on the review of literature it is evident that patient-centred care acts as a key factor in developing patient experience which later has a significant positive impact on patient satisfaction. As in other areas of health care, there would appear to be tension between what one group (health professionals) believe is best for patients, and that which patients themselves see as important. This is evident in the context of Saudi Arabia. Many healthcare professionals in the country are not aware of the positive impacts that patient-centred care brings. This lack of understanding of the patient-centred model for care is due to the societal norms in which doctors in the KSA believe that they know what is best for their patients and end up not formally including patients in their healthcare delivery process. This is of particular significance given how patient experiences can be positively influenced by the level of patient-centred care provided. At the moment, there is a relatively limited amount of literature on patient-centred care and how it impacts patient-perceived satisfaction (Nichols et al. 2013).
2.5.3 Measurement
Although patient satisfaction measures are widely used to assess the quality of care (Jagosh et al. 2011; Batbaatar et al. 2015), researchers lack consensus on how best to measure the construct. This difficulty seems inevitable given that it is challenging even to define the construct. A patient’s perceptions of their care are difficult to measure. Patient satisfaction is known to be related to their perceptions of hospital care and other items, and certain validated and reliable questionnaires have been developed to measure it. There is no one agreed questionnaire or instrument for the data collection on the subject. There is also the issue of construct validity, that is, is the researcher able to measure what they claim to be measuring? The problem with measuring patients’ conceptualisations of their experiences is not so much concerned with determining the factors that influence their views. Such factors are well known and established, as just indicated. The key challenge is to find a way for researchers to measure the patients’ attitudes to these identified factors in a reliable and agreed way. Therefore, in studying the relationship between patient satisfaction and perceptions of quality of care, it is essential to utilise robustly, validated, and reliable questionnaires.
Patient satisfaction is thus fundamentally different in health care settings compared to consumer marketing constructs, in which service experience approximates to expectations. Patient in a clinical setting tends to be indifferent concerning service quality and satisfaction, their focus is mainly on their treatment outcomes. It is only when expectations are not met that the patient is likely to judge the service quality as low (Kupfer and Bond 2012).
Indeed, ‘satisfaction’ must be a difficult concept to measure in any context. Against a background which sees the achievement of patient satisfaction as an important aspect of health care outcomes, Williams (1994) expresses concerns about the extent to which ‘satisfaction’ can be measured, let alone adequately defined. He argues that ‘satisfaction surveys provide only an illusion of consumerism, producing results which tend only to endorse the status quo (Williams 1994, p. 809). In effect, he suggests such surveys provide a veneer of patient involvement which may yield results that fail to reflect reality. For the meaningful experiences and perceptions of patients to be elicited, it is necessary that service providers first identify and isolate factors which provide true satisfaction to patients. In this regard, investigating practitioner skills and how they relate to patient satisfaction is critical for understanding the rationale for delivering good, patient-centred care. The method of the current study has been built upon this assumption. One of the aims of the study looks to comprehend the clinical effectiveness of health care (doctors’ and nurses’ skills, information provision, availability) effect on adult oncology inpatients’ satisfaction with care.
Some issues of major concern for researchers in this field have to do with the validity and reliability of results arising from satisfaction measurements. DuFrene (2000) suggests a solution to problems with validity and reliability in patient satisfaction measurements, namely, to adopt an extended survey to capture the opinions of patients. Merkouris et al. (2004), meanwhile, recommend using mixed methods, as they did in their study conducted in two large Greek hospitals. Interestingly, these two studies came to broadly similar conclusions: the highest levels of satisfaction were related to technical aspects of care, while the lowest had to do with information delivery.
Gill and White (2009) criticise the majority of research performed on patient satisfaction, questioning the validity of instruments used and highlighting associated underlying weaknesses and the subjective nature of patient satisfaction constructs. They indicate that using patient satisfaction as the measure of service quality is a flawed approach, which could hinder effective understanding of the quality of health services from patients’ perspectives. These researchers emphasise the need to focus on perceived service quality, differentiating it from satisfaction, and letting this inform the improvement of the delivery process in health care services. However, patient satisfaction measurements are still being used as a proxy for patient assessments of service quality (Turris 2005). For this reason, it is important to conduct further research on how best to define and measure patient satisfaction in healthcare settings.
There are common features of a patient's experience that are influential in the conceptualisation of their satisfaction, such as outcomes and communication. Patients’ attitudes to these can provide a good indication of how they conceptualise their experiences, once the data collection method is reliable and ensure a high degree of construct validity in the measurement of patient satisfaction. Promising instruments for assessing patient satisfaction have been developed. Whereas earlier studies on patient satisfaction were compromised by the use of invalid approaches to measurement, such as poorly established psychometric testing (William 1998), recent studies have found that certain satisfaction questionnaires/instruments have a well-grounded validity, indicating that developing reliable measures of satisfaction and perceived quality is possible. A good example is the measures of perceived quality described by Rao et al. (2006), which include medicine availability, medical information, staff behaviour, doctor behaviour, and hospital infrastructure. These dimensions provide a direct measurement of the ‘structure’ and ‘process’ of care.
One important issue, mentioned earlier, regarding the measurement of the satisfaction concept and quality of care, is the fact that evaluation of quality by the patient is difficult, especially about technical competence. For example, a physician who is perceived as action-orientated (e.g. requesting frequent blood or diagnostic tests) may be mistakenly viewed highly favourably (Kupfer and Bond 2012). In the current research, I recognise such limitations of patient satisfaction surveys and recommend adopting appropriate and evidence-based approaches.
In summary, there is considerable evidence demonstrating that patient satisfaction measures, are being extensively used as indicators of quality of care (Bredart et al 2007; Jagosh et al. 2011; Kupfer and Bond, 2012). The availability of different constructs of patient satisfaction is evidence of how complicated and challenging patient satisfaction is to measure. Patient satisfaction is very much related to patients’ perceptions of hospital care, and, in studying the relationships between these two constructs, it is important to utilise robustly, validated, and reliable questionnaires, which evaluate such constructs as separate dimensions.



Patient satisfaction in the KSA
This section discusses KSA-based research on patient satisfaction, particularly patients’ satisfaction with the quality of care provided to them. The current study uses the frequently cited dimensions of quality; safety, effectiveness, equity, patient centredness, efficiency, and timeliness in combination with process and structure to investigate how they impact a specific outcome which results in patient satisfaction. In order to further contextualize and justify the current study, this section of the literature review describes research studies conducted in the KSA on patient’s satisfaction with quality of care based on IOM’s 6 dimensions of quality.
The studies discussed in this section are summarized in the table below. After the table, structure and process of care are each discussed in separate sub-sections.
Table 2.1 : KSA studies on patient satisfaction and quality of care
Author-date | Sample | Methods | Key findings | Comments | |||
1 | Al Aloola & Al Bedawi (2008) Patient satisfaction in a Riyadh tertiary care centre. | 1983 inpatients, outpatients and ER patients | Cross sectional survey using self-developed patient satisfaction questionnaire | Patient satisfaction was noted in environmental aspect - room temp—etc. and less found in inter personal skills of doctors, phlebotomies, as they failed to introduce themselves. | ● The focus of satisfaction domain was only in socio-demographic context. ● No focus for specific service such as cancer, , which is a limitation ● Although it is valuable for originality, further research needed in cancer setting in the KSA | ||
2 | Al-Doghaither & Saeed (2000) Consumers' satisfaction with primary health services in the city of Jeddah, Saudi Arabia. | 75 patients aged over 15 years, chosen systematically | Self- administered questionnaire pilot test | Satisfaction scores were higher for patients that were assesses consolidated services, while individual service component were scored less. | ● Although high scores for satisfaction were noticed, service component need to be monitored too and assessed to provide satisfactory services | ||
3 | Saeed & Mohamad (2002) Satisfaction and correlates of patients' satisfaction with physicians' services in primary health care centers | n=540 patients in 8 PHC, selected randomly in Riyadh | Survey questionnaire, pilot-tested | Service items need to have correct measure. Also young adults and adult patients need emphasis | ● Other domain like hospital services, nurses’ skills would have an impact on satisfaction level of patients | ||
4 | Al-Ahmadi & Roland, M. (2005) Quality of primary health care in Saudi Arabia: A comprehensive review. | Systematic review of 31 papers met the inclusion | Reviews of literature | There were variations in quality of primary health care services in the KSA More effort needed in organisation of these services | ● Further research needed to address quality concerns from the patient’s perspective to have better insight into quality care | ||
5 | Mahfouz et al. (2004) Primary health care services utilisation and satisfaction among the elderly in Asir region, Saudi Arabia | 253 patients | In 26 PHC in ASIR (6 urban and 20 rural centres), House-to-house survey by interview with expert health worker, Arabic speaker, to answer survey questions Questionnaire address 5 aspects of services adopted from Mansour and Al-Osaimi study 1993 (continuity of care, humanity, accessibility, thoroughness and information). | Satisfied patients reported but 79% dissatisfaction found in 3 items: lack of audio-visual for patient education, lack of enough specialty clinic and prolonged waiting time in centres. | ● Emphasis on 5 aspects lack reasoning ● More concerns needed in evaluating different socio-demographic characteristics in elderly patients - results will be significantly different from area to area so such a comparison would be desirable | ||
6 | Akhtar & Nadrah (2005) Assessment of the quality of breast cancer care: A single institutional study from Saudi Arabia | 78 operable breast cancer patient | Retrospective analysis of breast cancer patient charts and histopathology reports from 1995-2000 | Only 37% had triple assessment before surgical procedure radiotherapy not used as per required standard overall conclusion that quality below international standard | ● No socio-demographic data were retrieved for their sample, which was a limitation that could be addressed in future research | ||
7 | Ibrahim et al. (2002) Appraisal of communication skills and patients' satisfaction in cross-language encounters in oncology practice. | 255 patients | Questionnaire “Art of Medicine” used to assess patients' perceptions of clinicians' communication behaviours and patients' global satisfaction. | No difference - means that language doesn’t affect interpersonal skills like communication and patient satisfaction. Patients were equally satisfied in both languages. | ● Interesting finding but the scale used was not described clearly.
| ||
8 | Alahwal et al. (1998) “Cancer patients’ awareness of their disease and prognosis”, Annals of Saudi Medicine, Vol. 18 No. 2, pp. 187-9. | 136 (33 cancer patients, 63 doctors, and 40 laypeople) | Questionnaire of 4 questions developed for the purpose of this study Distributed in western region of Saudi Arabia (major hospital providing cancer care) | All patients were in favour of being given full information regarding cancer; this would help them have a better understanding of how to deal with their illness. Doctors too favoured that the patients be disclosed about their conditions. | ● Although patient views were taken, the methods would be more useful had qualitative interview been used as this provides expanded insights into communication issues with patients | ||
9 | Younge et al. (1997) Communicating with cancer patients in Saudi Arabia | None | By literature review on communication aspects and factors influencing communication in the KSA | Communication influenced by many factors such as cultural and social and also health services that lack community care for chronic illness. | ● Number of studies reviewed was not mentioned and this generalisation potentially limits the findings. | ||
10 | Mansour and Al-Osimy (1996) A study of health centres in Saudi Arabia | 300 Consumers | Assessment sheet of centres’ resources in terms of quality and availability and consumer satisfaction & a 4-point system likert scale to measure satisfaction in 5 domains: continuity of care, accessibility, humaneness, information and thoroughness. | Discrepancy of data has been found between centres’ resources evaluation and those from consumer satisfaction results | ● More studies needed to evaluate resources and satisfaction through valid measures. ● Studies in hospital resources can provide further insight into patient satisfaction since they focus only on health centres. | ||
11 | Almuzaini et al. (1998) The Attitude of Health Care Professionals toward the availability of Hospice Services for Cancer Patients and their Carers in Saudi Arabia | 695 (398 health care professionals, 136 cancer patients and 161 informal carers) | Quantitative survey of participants on the quality of health care | The Ministry-owned or managed facilities score poorly on patient satisfaction with service organization. | ● Further research needed using a valid tool to determine which aspects of patient satisfaction are relevant or important to cancer patients while addressing the area of improvement in government facilities. | ||
12 | Brown et al. (2009) Failure to attend appointments and loss to follow-up: a prospective study of patients with malignant lymphoma in Riyadh, Saudi Arabia | A 3-year prospective study of 199 patients with malignant lymphoma in Riyadh | Retrospective analysis of No Shows appointments (No Shows=340 ) | 34% were related to hospital-based communication errors. 17.6 % were related to errors in patient communication with hospital | ● Based on retrospective analysis which need further empirical research to understand communication problems | ||
13 | Jazieh, A.R. (2010) Human resources development , ‘Initiative to Improve Cancer Care in the Arab World’ | 12 Experts in health care from across the Arab world and international experts | Interviews, situational analysis | There is lack of high-quality and well-trained health care professionals | ● The research based on only situational analysis. So, further robust methodology required to evaluate the needs of human resources in cancer | ||
14 | Saghir & Azim (2010) Standards of Care and Guidelines for the Arab World with Limited Resources | 12 experts in health care from across the Arab world | Panel discussions | Lack of standardisation in doctors’ and nurses’ skills leads to varying quality. | ● The research is based on panel discussion and does not use any objective methods or criteria. | ||
15 | Diab, R. (2010) Access to Cancer Care Facilities, ‘Initiative to Improve Cancer Care in the Arab World’, | 8 panel members made of experts in policy making, healthcare and scholars (a | Panel discussions (Based on discussion of panel members about priority of objectives and available baseline information of accessibility to cancer care) | The panel found that quality of cancer care suffered from problems like long wait times for the patients, high costs, and lack of access to health care and inequality in access for people from rural and marginalised regions. | ● No mention of criteria for evaluating the health care facilities, such as introducing use of measures or indicators of quality. | ||
16 | Shamieh et al. (2010)Access to palliative care | 12 multi-disciplinary experts in palliative care | Panel discussion | Access to cancer care is poor compared to palliative care | ● Discussions purely based on the perceptive of the experts. Patient views are needed to allow comprehensive evaluation of the issue | ||
17 | Al-Faris et al. (1996). Patients' satisfaction with accessibility and services offered in Riyadh health centers. | 466 randomly selected patients from 6 randomly selected primary health care centres PHCC in Riyadh City | Patient satisfaction and attitude survey | The research found high level of satisfaction among older patients, housewives and non-Saudi patients. | ● The questionnaire was self-administered, which may add to bias. | ||
18 | Al-Sirafy et al. (2009) Hospitalisation pattern in a hospital-based palliative care program: An example from Saudi Arabia. | 759 palliative patient admissions during a 4-year period (in the absence of sub- acute palliative care models) | Retrospective review of palliative admissions were studied for reason for hospitalisation, duration of stay and mortality rate | The research found that quality of life did not improve with palliative care in Saudi Arabia. The indicators of quality for palliative care included factors like duration of stay and mortality and quality of life. | ● While factors like mortality etc. were easy to understand and calculate, there was no elaboration on factors that may indicate the quality of life improvement. | ||
19 | Aljubran, A. (2010) The attitude toward disclosure of bad news to cancer patients in Saudi Arabia. Annual Saudi Med, March April. 2010 | None | Literature review | The researchers highlight the changing trends in patients’ need to understand and know their illness. | ● Cultural shift toward considering patient perspective in Saudi culture is evident and warrant further exploration | ||
Few studies were found which focused on the quality of hospital-care in the KSA, and most research that deals specifically with the country was shown to be focused on the quality of primary care services (Mansour and Al-Osimy 1996; Alahmadi and Roland 2005; Al-Doghaither and Saeed 2000; Al-Faris et al. 1996; Saeed and Mohammad 2002). Results from these studies demonstrated wide variations in quality of care in the primary care setting, and all recognised the need for further research.
One study of note assessed patient satisfaction in a tertiary care centre in the KSA (Alaloola and Albedaiwi 2007), and another focused on quality of cancer care, specifically, assessing the quality of breast cancer care in a KSA health care institution (Akhtar and Nadrah 2005).
Notably, certain studies that used quantitative methods, based on patient satisfaction surveys or opinions of health care experts, appeared to have a number of flaws. Although the review included the studies assessed as robust, there were some weaknesses in study design or methodology, for example, small sample sizes, retrospective analysis, use of non-validated tools or poor transferability of results (Akhtar and Nadrah 2005; Alaloola and Al Bedawi (2008); Saeed and Mohamad (2002); Mahfouz et al. (2004). Also, there has not been any previous KSA empirical study that has focused specifically on patient satisfaction in oncology settings. It is also worth noting that there has not been any previous qualitative study that has explored the issue of patient satisfaction in KSA.
Despite a paucity of published literature and some flaws in the existing research in the KSA, there is a general, overall trend evident across the published literature. That is, there was evidence that patient satisfaction was adversely affected by (1) poor access to care and treatment availability, (2) poor service coordination between different units and professionals, (3) lack of communication within the multi-disciplinary team required for oncology care, (4) lack of patient communication and awareness, and (5) a general lack of adherence to standardised guidelines related to diagnosis, treatment and monitoring of cancer patients (Akhtar and Nadrah 2005; Al-Doghaither and Saeed 2000; Almuzini et al. 1998; Younge et al.1997; Brown et al. 2009; Diab 2010; Shamieh et al. 2010).
To date, research on patient satisfaction in the KSA suggests that patient satisfaction generally varies according to various factors, in particular, the age of the patient (Al-Faris et al., 1996) and the healthcare providers’ disclosure practices (Al Ahwal et al. 1998; Younge et al. 1997; Aljubran 2010; AlAmri 2009).
.2.6.1. Structure
The structure of care involves the manner in which a patient accesses and receives care. The way that care is provided and structured is important, particularly with respect to how patients conceptualise their satisfaction with their experiences in a health setting. A retrospective study by Al-Sirafy et al. (2009) indicated the need to improve access to palliative care services in the KSA, and revealed that patients could not identify evidence of improvement in their quality of life or health. Al-Muzaini et al. (1998) also found that improvements in structure and the manner of delivery are challenged by the lack of knowledge of evidence-based cancer care, and by drug shortages. It was concluded that there is a need for provision of an effective framework for palliative care services in the KSA health system.
The recent widespread recognition by Arab countries that the status of palliative care is poor and lacking in structures has given rise to the ICCAW initiative (Initiative to Improve Cancer Care in the Arab World). As part of this initiative, Shamieh et al. (2010) led a panel of experts tasked with recommending modifications to the Comprehensive Cancer Network (NCCN) Guidelines. These guidelines made various suggestions for improvements in the structures of palliative care provision. Shamieh et al.’s (2010) report also concluded that there was little research data from the KSA upon which to recommend changes.
In terms of access to services, Diab (2010) was tasked with finding out how to improve access to cancer care facilities, with the objective of identifying key issues, including concerns about excessive waiting times, prevention and screening, diagnosis and treatment, quality of life, and palliation. The findings were clear that there are problems with regard to the structure for the delivery of, and access to care in the different Arab countries, including the KSA. The need for an initial assessment to develop a database of baseline information for cancer care facilities was identified.
Lack of satisfaction from a patient’s perspective has been reported in a number of other KSA studies that evaluated various dimensions of the quality of care. Mansour and Al-Osimy (1996) identified patients’ dissatisfaction with the resources and care provided, whilst Al-Ahmadi and Rolands (2005) identified poor access to adequate chronic disease management programmes and inadequate health education, along with ineffective systems for referral and for prescribing. Research in breast cancer tertiary care health care institutions also indicated dissatisfaction with the quality of the general standards of cancer care and the significant underuse of radiotherapy; both were recognised as being below internationally accepted standards (Akhtar and Nadrah 2005).
A major study in the KSA, conducted by Alaloola and Albedaiwi (2008), highlighted that patients’ perspectives on service delivery are a core service quality indicator. Their study focused on the level of patient satisfaction or dissatisfaction in a tertiary centre in Riyadh using a cross-sectional survey of 1,983 inpatients, outpatients, and emergency care patients. It was the first report of service quality and patient satisfaction of the KSA health care systems to appear in a peer-reviewed journal. One limitation of this otherwise invaluable study was that not every service was studied separately, so the patients’ answers may not represent any one hospital setting. The researchers recommended that further studies on patient satisfaction in the KSA are needed.
There is also a need to explore related aspects of cancer treatment within the KSA, including unacceptable side effects (like osteoporosis) caused by current chemotherapy drug use (Al-Amri and Sadat, 2009), and the need to focus on the significant number of patients failing to attend medical appointments (Brown et al., 2009). In the study by Brown et al. (2009) in Riyadh, which involved patients with malignant lymphoma, communication problems were responsible for 34.1% of missed appointments, while another 17.6% were found to be the result of patient communication errors. One area identified as problematic was the movement of patients with limited access to outpatient appointments and hospital facilities. Addressing such problems represents an essential role of a service organisation.
These studies demonstrate the potential for considerable patient dissatisfaction with certain structural aspects of healthcare in the KSA and, hence, the need to further investigate patient perceptions of a range of specific key indicators of service organisation in the KSA. It should also be emphasised that much of the data presented from the KSA are not derived through primary research, but arise from retrospective analyses of data from patient files or records. The need for robust, reliable evidence from empirical research provided a rationale for the current study to examine the quality of patient care in oncology wards in the KSA.
2.6.2 Process
Research suggests that the processes by which healthcare is delivered in the KSA are inconsistent in nature and quality, which may give rise to inconsistencies in patient satisfaction. A lack of consistency in the quality of the clinical care processes has been clearly identified in the KSA. Research in Riyadh (Saeed and Mohamed 2002) established that the patients were largely satisfied with the doctors and the nurses, but this research was undertaken in a context where experienced Muslim physicians and an Arabic-speaking health team were offering free services near patients’ homes. The findings of the current study may not then be generalizable with regard to patient’s conceptualisations of their satisfaction in the KSA.
A number of studies have also shown high levels of patient satisfaction in other specialties. The study by Mahfouz et al. (2004) showed that elderly patients were largely satisfied with the doctors and the health care givers’ attitudes and behaviours, but patients were generally dissatisfied with long waiting times, lack of speciality care, and lack of information provided to them. Al-Faris et al. (1996) studied primary health care centres (PHCC) in Riyadh and found that the satisfaction levels varied according to the factor investigated. Although patients were generally satisfied with the service provided and with the respectfulness of the staff, they were significantly dissatisfied with the interpersonal skills of some health care staff and with poorly explained procedures.
The KSA’s Ministry of Health regulates both the governmental and private health sectors. The Ministry of Health has the capacity to set standards for national-level strategies for health reforms through change management and allocation of financial resources. Raising the health level of the population is informed by the government’s health research, which is included as a strategy within the National Health Program/Plan. In 2005, Al-Ahmadi and Roland (2005) acknowledged that there was a deficit in the literature on the effectiveness of quality primary care in the KSA, even though the Ministry of Health argued that high quality of care is a key to the national health strategy. The available evidence shows that clinical effectiveness in the KSA has historically been considered to be low.
A study of satisfaction among primary health care patients in the KSA by Mansour and Al-Osimy (1993) indicated low satisfaction with the quality of care of the referral system. More recently, research has showed that patients have developed poor perceptions of the effectiveness of primary health care in the KSA (Al-Ahmadi and Roland 2005). Ineffectiveness and inefficiency in primary care were reported in relation to disease management programmes, prescribing patterns, health education, referral patterns, and some aspects of interpersonal care, including those caused by language barriers. In addition, Al-Ahmadi and Roland (2005, p. 331) also identified other determinants of the ineffectiveness of primary care such as ‘poor management and organisational factors’, ‘poor implementation of evidence-based practice’, ‘low professional development’, ‘lack of structured approach to use of referrals to secondary care’, and ‘use of healthcare professionals that were not sensitive to the culture of Saudi Arabian patients’.
Hopeful changes are underway in the KSA. Recently, a report by the Ministry of Health (MOH 2010) identified failures in health care in the KSA, which were largely people-related and not technology-related; they were also linked to complexities in management of health information (Ministry of Health, MOH 2010). This led to a Ministry drive towards improvements in primary care practice in a number of regions. One important and positive change has been the adoption of an e-Health approach, as part of the wider KSA focus on e-Government, aimed at improving the efficiencies and effectiveness of health care. The KSA’s use of e-Health has been identified as a strategic objective for the Ministry, which should not just improve health, but enhance how patients perceive the effectiveness of care and availability. The approach involves linking regional health directorates, hospitals, and hospital management centres. The KSA e-Health governance model claims to improve service design through alignment of health care with dimensions of quality of care, management of relationships (doctor-patient relationships, nurse-patient relationships), and by ensuring delivery of value to patients. However, despite this drive to provide high-quality health care services in the KSA, evidence of patients’ perceptions of quality care in the KSA is lacking, and a gap in the knowledge remains. These findings highlight the need for research on patients’ concepts of satisfaction as one of the key indicators of quality of care from the perspective of clinical effectiveness. Specifically, it would be pertinent to conduct research to investigate how doctors’ or nurses’ skills could be developed to help improve perceived clinical effectiveness of care and other care processes The current study will help achieve such objectives.
In order to determine a practitioner’s clinical effectiveness, the use of evidence-based practice is important. Evidence-based Clinical Practice Guidelines (CPGs) are important tools to help improve patient care and health outcomes. Al-Ansary and Alkhenizan (2004) conducted a review of CPGs and of the tools that have been employed in CPGs in Saudi Arabia for the last two decades. Their findings demonstrated the need for good quality, effective CPGs in the KSA to enable alignment with expected standards for quality of care. Ideally, to reduce work and costs, this could be accomplished through local adaptation of good-quality international guidelines. There is a dearth of information in the literature on the way CPGs could provide a basis for improving dimensions of care in the KSA. Recent studies have focused on quality measures/indicators which are known to improve care outcome. Al-Moajel (2012) showed how improving the effectiveness of quality of care relies on the development of hospital performance indicators in the fields of accreditation or the certification of health care structures and processes of care.
One potential problem identified in the KSA is accurate measurement of performance indicators. This is in line with the call by Bilimoria et al. (2009) in the US for a framework for policies and procedures to outline the best approach for such measures. In addition, there is a need for implementation of standardised, quality indicators in daily practice through effective strategies to reduce variability and enhance the level of improvement obtained (Vos et al. 2009). Indeed, Al-Moajel (2012) maintains that quality indicators are essential to improve the quality of health care services. Al-Moajel’s (2012) study also recommends accreditation of hospital care services as a step towards aligning quality of care dimensions with set standards, as part of clinical governance. Despite the clear need for such measures, there is currently no literature on how accreditation and certification systems in the KSA have affected patient satisfaction or impacted on clinical effectiveness.
2.7 Conclusion
This narrative synthesis approach to literature review has demonstrated the difficulty of defining and measuring quality of care and patient satisfaction. The review also demonstrated the gaps in current scholarship on patient satisfaction in the KSA.
A key element of this discussion has been the relationship between patient-centred care and patient satisfaction. This will be the main factors that are analysed in the current study using the mixed methods research approach as discussed at great length in chapter 3. The literature review has provided a direction for the current study by which research can be conducted to ensure that relevant information is drawn in order to provide meaningful results in terms of patient satisfaction that are discussed further in chapter 4, 5, and 6.
This review has evaluated the knowledge base of patient satisfaction, with particular focus on the oncology care setting in the KSA. By expanding the understanding and knowledge base of patient satisfaction in the KSA, this review has identified significant gaps in the research. This review has consequently provided justification for the current research, and given rise to the following research question:
What factors contribute to or hinder patient satisfaction with care in an oncology ward setting in a Saudi Regional Cancer Centre in Riyadh?
The identified gaps in knowledge highlighted in this review can be addressed by effectively interpreting the relationship between patient experience/satisfaction and quality of care, while maintaining a focus on oncology patient satisfaction in the KSA which is conducted for the current study. The ultimate intention of the current study is to contribute knowledge to a hitherto poorly researched area.
Chapter 3 - Methodology and Methods
3.1 Introduction
The literature review indicated the need for empirical research on patient satisfaction in the KSA, particularly patient satisfaction in oncology wards. As indicated in the review, it is important to address these gaps by exploring, understanding, and interpreting the influential processes in oncology patient satisfaction in the KSA. Studies from outside the KSA offer insights into ways in which patient satisfaction varies in different care settings internationally. However, few studies to date have explored patient satisfaction in oncology ward settings in the KSA. This indicates that there is a need to consider how, in the cultural context of the KSA, various influencing factors might determine satisfaction of care, and why and how a patient is satisfied or dissatisfied with the care provided in the KSA.
By focusing on this important gap in the literature the following research question was developed:
‘What factors contribute to or hinder patient satisfaction with care in an oncology ward setting in a Saudi Regional Cancer Centre in Riyadh?’
In this chapter the methodology and research methods selected to answer this research question and to meet the aims of the current study are outlined and discussed. A sequential mixed methods approach was used for this research, to answer most effectively the research question and to address the aims of the study. The first, quantitative phase of the research provided data from questionnaire responses. The results of the analysis of this data were then used to inform the second, qualitative phase which employed semi-structured interviews.
Following this brief introduction, the research question and study aims are considered in more detail before the rationale for the study design is presented. Additionally, the theoretical reasons for using a pragmatically informed, mixed-method design to explore the complex and multifaceted issues of patient satisfaction in the KSA are discussed. The chapter continues by providing a detailed description of how the study was conducted; this includes a description of the study setting, the procedures for recruiting and selecting patients, and the means of data collection and analysis for the two phases. The chapter concludes with an exploration of the ethical issues associated with the current study and a description of how these were addressed.
3.2 Research question and study aims
The primary research question driving the current study was as follows: What factors contribute to or hinder patient satisfaction with care in an oncology ward setting at the Saudi Regional Cancer Centre in Riyadh (SRCC)? This primary question was broken into three more specific sub-questions to be answered during Phase 1:
- Does the clinical effectiveness of health care (doctors’ and nurses’ skills, information provision, availability) influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
- Does accessibility to health care (service organisation) influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
- What are the socio-demographic characteristics of adult oncology inpatients at the SRCC in Riyadh?
Informed by the responses in Phase 1, another series of specific questions was asked during Phase 2:
- How do interpersonal aspects of care influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
- How do socio-cultural communication factors influence adult oncology inpatients’ satisfaction with care at the SRCC in Riyadh?
The specific aims of the study were as follows:
- To determine the likelihood that clinical effectiveness is associated with patient satisfaction in adult oncology ward settings in SRCC.
- To determine how likely the accessibility to health care is associated with patient satisfaction in adult oncology ward settings in SRCC.
- To describe the characteristics of patients in adult oncology ward settings in SRCC.
- To explore the extent to which interpersonal aspect of care influence patient satisfaction in adult oncology ward settings in SRCC
- To provide recommendation for enhancing patient satisfaction in oncology ward settings in KSA
- To discuss the extent to which and in what ways the qualitative findings help to explain the initial quantitative results of patient satisfaction in oncology settings in KSA
3.3 Research methodology: Overview of mixed methods
The use of a mixed-method design enables quantitative and qualitative methods to complement one another and allow for a more thorough analysis of the research problem (Creswell 2003). As the purpose of the current study is to explain the impact of various factors on a patients’ satisfaction in oncology wards in KSA, the mixed-methods design is best suited for the research. This sequential mixed methods design was chosen for various reasons; which will be justified throughout the current chapter. Firstly, the research problem is qualitatively-oriented; a rational qualitative instrument was used to gain insight into the various factors that may influence patient satisfaction. Secondly, the results of the quantitative research are thought to aid in explaining and gaining insight into the qualitative findings (Creswell and Plano-Clark 2011).
Creswell and Plano-Clark (2011) have argued that the use of combining qualitative and quantitative approaches provides amore absolute and complete understanding of the research problem than the use of only a single method. It is true that a quantitative method is able to identify the variables that are systematically or statistically correlated, but the method fails to provide insight into the reason why the variables are related in the first place. Furthermore, Polit and Beck (2008) states that a qualitative explanation can clarify the imperative ideas and substantiate the findings from the statistical analysis, and also provide guidance that helps in the interpretation of results. Therefore, the researcher had chosen the integration of the two methods to provide a more robust understanding of the research problem as either methods would be inadequate to do so alone.
3.3.1 Key issues in mixed methods research
Mixed methods research is where quantitative and qualitative techniques are combined in a research project and the level of interaction between the techniques used. The method is based upon the premise that such a mixture of quantitative and qualitative methods is both practical and compatible. A mixed methods approach can help the researcher to overcome problems in the collection of data and provide reliable findings as quantitative results provide concrete statistical facts which are supported through detailed insight provided by qualitative findings (Creswell 2003). The combining of the two research methods namely, quantitative and qualitative complement each other and the data collected can be integrated and also limits the weaknesses in each separate technique as discussed above.
According to Creswell and Tashakkori (2007 p.4) mixed methods research can be described as:
“Research in which the investigator collects and analyses data, integrates the findings and draws inferences using both qualitative and quantitative approaches or methods in a single study”
Some researchers claim that MMR results in clarity in understanding the complexities of the social phenomena that are under investigation (Ponterotto and Greiger 1999).
There are several benefits in using a mixed methods approach to research, namely, (1) triangulation (using multiple data collection methods to corroborate findings and to validate these methods); (2) complementarity (elaborating, and clarifying the results of one method using another); (3) initiation (uncovering contradictions that lead to re-framing the research question); (4) development (using the findings from one method to inform the other); and (5) expansion (expanding the breadth of research by using different methods at different stages of research) (Greene et al. 1989).
Some of the strengths of mixed methods designs that have been of particular benefit to the current study are that (1) interviews have extended and deepened the survey data, and (2) the conclusions of the study were stronger due to the synthesis of the findings from both methods, thus strengthening the recommendations for improvements to enhance patient satisfaction. There are, however, certain weaknesses in the use of MMR. Using different methods can result in different types of answers to a research question. Moreover, a practical limitation is the amount of time required to conduct such a study (Creswell 2009).
The MMR method needs a research paradigm to provide a framework for the research to be able to adequately address the research questions. Creswell and Tashakkori (2007) maintain that a research paradigm represents a belief system or theoretical assumptions and propositions that provide guidelines on how to answer a research question. Four foundations of research paradigms exist, namely, (1) positivism (built on experimental testing); (2) post-positivism (viewpoint arising from the need for a research context and a recognition of the insufficiency of context-free experimental designs); (3) critical theory (viewpoint that ideas relate to specific ideologies, and biases ought to be articulated; and (4) constructivism (viewpoint that every individual researcher creates his/her independent reality, and therefore, multiple interpretations exist).
According to Sale (2002), ‘one cannot be both a positivist and an interpretivist or constructivist’ (Sale et al. 2002 p.47). Similarly, Hammersley (1996p.160) argues that:
Quantitative and qualitative methods have been presented as opposing paradigms, to be used as and when appropriate, depending on the focus, purposes and circumstances of research
The primary question of this debate is whether, when using quantitative tools in a mixed methods design, one adopts a positivist interpretation, or whether the overall research design remains constructionist or interpretivist. The latter position implies that use of quantitative data collection tools means it is still important to develop conclusions using constructivist approaches.
The logic behind the use of MMR in the current study is driven by practical considerations such as study design, skills and resources as well as theoretical reasoning (i.e. study aims) (Bryman 2006). The primary aim and research question of the current study is to establish a relationship between how the factors uncovered impact patient satisfaction. Keeping in mind the primary aim it is evident that it is necessary to comprehend which major factors influence patient satisfaction which can be revealed through a quantitative measuring instrument, in this case a survey. However, to fully comprehend the factors further insight is needed in terms of understanding patient opinion on the healthcare delivered to them and ultimately how that impacted their satisfaction. This is consistent with the perspectives of Snape and Spencer (2003), who argue that ‘quantitative and qualitative methods can and should be seen as part of the social researcher's ‘toolkit’ (p.15). This view echoes work by Feilzer (2010), who maintains that methodological choices should be based on the aim of the study.
While Onwuegbuzie and Leech (2005) and Creswell (2009) stress the importance of pragmatism in MMR, some researchers maintain there is still lack of clarity in how pragmatism can shape and define the mixed methods approach (Tashakkori and Teddlie 2003). Nevertheless, the general consensus in the literature is that some versions of pragmatism represent the most useful philosophy for supporting MMR. For example, Johnson et al. (2007) contend that pragmatism is a suitable philosophy for integrating different perspectives and mixing approaches through application of epistemological justification and logic. According to Johnson et al. (2007), by mixing approaches and methods, the outcome would more readily be able to address and provide tentative answers to one’s research question(s). Similarly, Morgan (2007) provides a holistic view, describing how researchers can vary their approach depending on the research question and draw on pragmatic approaches as a philosophical and practical basis for conducting MMR. This approach enables a multiplicity of perspectives, which enables a deeper understanding of the research problem (Eaves and Walton 2013). Therefore, the current study adapts pragmatism as philosophical framework underpinning this mixed methods research.
Notably, it has been asserted that neither qualitative nor quantitative methods alone are adequate or robust enough to provide a complete analysis of the complex nature of research in areas such as health care (Sale et al. 2002). This is especially true in this investigation of patient satisfaction in an oncology setting in the KSA since cultural, political and communication problems may all play a role, yet may be difficult to explain through using either a survey or interviews alone. This is at the heart of my decision to use a MMR design which has already been successfully used to understand patient satisfaction in other studies (Hyrkaas and Paunonen 2000; Merkouris et al. 2004). Moreover, an important advantage of mixed methods is that it allows triangulation between two or more types of data to assess the same problem, so that different perspectives can be corroborated, thus giving weight and validity to the interpretation of the results (Green et al. 1989; Bowling 2007). The convergence of two or more datasets increases confidence in the results (Bogdan and Biklen 2006). Complementarity uses the results of one research method to elaborate or clarify the results of another, thus achieving a fuller understanding of the phenomenon (May et al. 2000; Sale et al. 2002; Creswell 2003; Bowling 2007). One practical issue of complementarity is the sequencing between the phases and whether the quantitative and qualitative methods are adopted simultaneously or sequentially (Creswell 2009). A common approach suggested by Bryman (2006, pp.106) is that corroboration through the use of qualitative data helps to ‘put meat on the bones of dry quantitative findings’. However, Pope and Mays (1995) emphasise a key point about using qualitative research to corroborate quantitative research in a mixed method study:
…is not simply a matter of joining two techniques, or tacking one on the end of a project. Researchers need to be aware of the different types of answers derived from different methods (Pope and Mays, 1995, p.44).
An alternative approach to combining data is described by Creswell (2009), namely, the explanatory design. The explanatory design involves two-phases where qualitative data helps to explain and expand upon initial quantitative results (Creswell et al. 2003), and is especially useful when such data is needed to explain significant/non-significant results, or outlier results (Sale et al. 2002).
3.3.2 The applicability of explanatory mixed methods to this research
The following four key factors were examined as proposed by Creswell (2009) to determine if the MMR methodology was warranted for the study:
Timing
The collection of qualitative and quantitative data may be scheduled and timed so that the data are collected simultaneously or sequentially. As shown in the current research questions, the sequential data collection methods was adopted within both phases. According to McNabb (2012) the strength of a survey is identified with its ability to collect large amounts of responses over a specific period of time and its ability to represent the target population. In the current study, a reliable and validated instrument (phase 1) was used and then followed with semi structured interviews to examine the factors influencing patient satisfaction (phase 2) of cancer patients in SRCC.
Weighting
Weighting refers to the priority and emphasis given to both the qualitative and the quantitative methods. Giving greater emphasis to the quantitative method was necessary to ensure that the maximum amount of data was collected and analysed prior to seeking explanation by using interviews in the qualitative phase allowing to keep focus on its application.
Mixing
Mixing involves merging two forms of data into a structure that allows for reliable evidence to be drawn upon with relation to the research question and aims. Mixing in the current study involved analysing the complementary quantitative and qualitative data sets and then combining the findings from both into the study.
For the current study mixing was conducted by analysing the qualitative data and then using the conclusions from that data to support the quantitative data. The two sets of data were complementary and could be combined to provide information on the complex construction of patients’ concepts of their satisfaction.
Theorising
Theorising requires consideration of whether mixed method research is suitable for the chosen research paradigm – the pragmatic paradigm in this instance. The MMR methodology was deemed suitable because it could generate a large amount of data from different perspectives which was needed to represent and understand how the patient constructed satisfaction with their care.
MMR methodology was deemed to be appropriate for this kind of research and is justified with respect to the ten criteria suggested by the Health Foundation ‘when planning how to measure patients’ experience’ including satisfaction (Health Foundation, 2013, p. 28). The current research meets the Health Foundation criteria as follows:
- The term patient satisfaction was defined in ways that can be assessed by both quantitative and qualitative data.
- The patient satisfaction being measured allowed for a good understanding of how patients construct their experience and it was possible to use data on their responses in this respect to answer the research question.
- It was considered useful to combine both qualitative and quantitative data in order to maximise the data collected.
- The MMR method was suitable as it enabled samples to be selected rather than all the general population, which was impractical in a study of this size. The MMR approach allowed the researcher to draw from the samples the maximum amount of data possible.
- The MMR method allowed for a significant amount of data to be collected within a tight time frame. This helped to address the particular challenge that I faced of a limited period permitted for field work
- The MMR methods used were tested before they were implemented and they are all well established and proven data collection instruments as used in previous patient satisfaction studies (Hyrkas et al. 2001;Merkouris et al 2004).
- The data collected by MMR methods could be merged in such a way as to allow the information to be analysed robustly and reliably.
- The MMR methodology was chosen because it could present information in a suitable way for the intended audience.
- The MMR methodology allowed people to express their opinions freely and to feel comfortable providing information to the researcher.
- As there is no single measurement of patient satisfaction, there needs to be several ways of measuring it. Therefore, by providing more than one perspective, the MMR can provide the data needed to address the research question (Health Foundation, 2013, p. 27).
3.3.3 Summary of the MMR approach taken
The primary research question of the current study focuses on the factors that contribute to or hinder patient satisfaction with care in an oncology ward setting in a Saudi Regional Cancer Centre in Riyadh. The use of sequential mixed methods design was considered the most appropriate for reaching the aims of the study and answering the research questions.
Accordingly, in the current study, an explanatory approach was adopted, but with complementarity in mind, whereby the patient satisfaction survey was conducted first and, after analysis of the quantitative data, one-to-one interviews (both by phone and face-to-face) were carried out with oncology patients to provide an assessment of patient satisfaction and assess the relationship between the various factors identified and connected to patient satisfaction. As this method is applicable in both the social and health disciplines, the methods was considered as most appropriate for assessing the relationships between variables that influence patient satisfaction for patients in oncology wards in KSA (Creswell and Plano-Clark 2011). Integration takes place at the intersection of quantitative phase1 and qualitative phase 2. The qualitative Phase 2 interviews explore further the quantitative Phase1 results in order to provide deep understanding of patient satisfaction. Figure 3.1 shows the visual model of the explanatory mixed method design used in the current study.
In summary, the sequential explanatory mixed methods approach provided an explanation of the findings that are later identified in the quantitative phase, by a set of participants using semi- structured interview questions. The data allowed for a richer understanding of the relationship between patient satisfaction, patient experience, quality of care, and health care delivery for oncology patients in SRCC, KSA. The findings of the current study are expected to provide a significant contribution to the literature of patient satisfaction and patient experience to improve healthcare service delivery in KSA.
Figure 3.1 The visual model of explanatory mixed methods design used as adapted from Creswell (2009):
|
|
| QUAN | → | qual |
|
|
|
QUAN |
| QUAN |
| qual |
| qual |
| Interpretation of Entire Analysis |
Data | → | Data | → | Data | → | Data | → | |
Collection |
| Analysis |
| Collection |
| Analysis |
|
3.4 Phase 1: Quantitative method
3.4.1 Quantitative design: Cross-sectional survey
The first phase of the study comprised a quantitative, cross-sectional survey. According to Hennekens and Buring (1987), a cross-sectional survey examines the relationship between disease, or other health state, and other variables of interest that exist in a defined population at a single point in time. Cross-sectional studies are descriptive in nature. For example, they are used to describe certain characteristics of a population, such as prevalence of illness, or they may be used to support inferences of causes and effects (Rothman & Greenland 1998).
Phase 1 of the the current study involved a cross-sectional survey of an adult oncology inpatient group. It was administered to determine their levels of satisfaction with the care provided to them at the time of their participation. A validated EORTC IN-PATSAT 32 Questionnaire (the inpatient satisfaction quantitative questionnaire, as developed by Bredart et al. (2005), was therefore distributed to adult oncology inpatients in a Saudi Regional Cancer Centre in Riyadh. This questionnaire was deemed a reliable data collection instrument as it has a track record of being used in similar research (Arrora et al. 2010; Obtel et al 2012) and it has been designed to provide information on patients in an oncology setting which was the context for the current study. Section 3.4.5 describes the questionnaire in details
The setting of the current study was adult male and female oncology wards in one of the main KSA regional referral cancer centres in Riyadh (SRCC). The bed capacity of the oncology wards is a total of 42 beds. This setting was appropriate, as the centres admitted adult male and female patients with varying types of cancer. Geographically, this area included a diverse population from which potential participants of various ages, and socio-demographic and cultural backgrounds could be sampled. This sampling was done to ensure that the data collected was not only representative of the inclusion and exclusion criteria detailed below.
3.4.2 Sampling strategy
3.4.2.1 Population
The population of interest for the current study was all adult male and female inpatients admitted to the SRCC in Riyadh.
3.4.2.2 Inclusion criteria
All participants in the research were required to meet the following criteria:
- Had a confirmed diagnosis of cancer
- Was aged 18 years or older
- Had been hospitalised for at least three days (to maximise number of patients)
- Was mentally fit to answer the questionnaire
- Was aware of their medical condition
3.4.2.3 Exclusion criteria
Likewise, those who met the following criteria were excluded from the research.
- Was unaware of their diagnosis
- Was aged less than 18 years old
- Had been hospitalised for less than three days
- Was unaware of their medical condition
- Did not wish to participate
3.4.3 Recruitment procedures
Following ethical approval from the University of Stirling, School of Health Sciences’ ethics committee, and from the Saudi Regional Cancer Centre (SRCC) ethics committee, I initiated contact with the clinical site in Riyadh. Senior managers, including the oncology nurse managers, head nurses in adult oncology wards, and the medical director were contacted to provide them with an explanation about the study’s aims and methodologies, and to enlist their assistance.
Recruitment and consent took place on the ward by direct contact with oncology ward staff, this personal approach was considered best, to secure cooperation and the help of the staff. One nurse educator in particular was responsible for distributing the questionnaires and surveys on the researcher’s behalf. Patients were given an information sheet and an invitation to participate (see Appendix 7 for the patient information sheet). They were given time to consider whether they wished to participate and to discuss this with their relatives. Those interested in participating were informed of opportunities to be selected for a follow-up interview for the qualitative phase of the current study
I communicated the criteria for inclusion and exclusion of potential participants to the nurse educator leading to her being aware of those criteria. Consequently, she was able to determine those eligible to participate and distributed the questionnaire to those who met the criteria.
An invitation letter, along with an information sheet, was distributed to eligible patients, who had a confirmed diagnosis and those who wished to participate stated their intention to the nurse educator depending on who was present in the ward. Patients took one to two days to state their intention to participate. Patients who agreed to answer the questionnaire were asked by the nurse educator to sign the consent form (see Appendix 8 for the patient consent form). Patient information was entered into a recruitment log to maintain the transparency of the research process. The recruitment log included a non-identifiable number for all participants and the following: age, gender, date of admission and the date of data collection were coded. The log facilitated the anonymity and confidentiality of the received data, and also managed the time scale for the recruitment process (see Appendix 9 for the recruitment log). The recruitment continued until a target of 100 patients who consented to participate was attained.
When the questionnaires were issued I was passed the details of those willing to be approached to be interviewed. The questionnaire itself informed the participants the procedures they needed to undertake, if they were interested in participating in the study. A contact number was provided and the potential participant could, or someone acting on their behalf could contact me using a number on the questionnaire. This allowed the participant to arrange a second interview for the qualitative phase of the study.
Since I am a native of KSA, I was very sensitive to the cultural issues in the collection of data, particularly patients’ cultural expectations. Privacy and respect for their opinions was considered essential and this was deemed necessary to ensure the cooperation of the sample population. Therefore I assured the potential participants know that their privacy was respected and that all of their responses would be treated confidentially. In order to ensure that patients understood the research process and that their participation was kept confidential it was essential to explain to each of the participating patients the purpose of the study. This included highlighting to patients how their input and opinions can contribute to the study. Furthermore, patients were informed that all information regarding their illness, diagnosis, and other personal information will not be included in the current study and the patients’ participation will be kept confidential.
During the initial data collection phase, there were certain limitations that became apparent. The relatively small sample raised issues over acquiring adequate data to analyse. Also, generalising the conclusion drawn from the data formed another limitation to develop a general theory of patient satisfaction. That is, the question of how (and to what extent) the findings from this location were representative of the general levels of satisfaction of oncology patients in the KSA receiving such care. There was also the issue that this was the first study of its kind. This meant that there were no previous examples to base the research upon and no way to learn from others’ experiences and indeed the limitations of such studies. A further limitation was caused by the restricted time available for conducting the research.
However, the findings are generalizable in the sense that the Saudi system is becoming more westernised and this means that the findings are more generalizable to oncology patients internationally. Research conducted elsewhere was a useful resource that helped to guide me the collection and analysis of data.
3.4.4 Sampling methods and response rate
A convenience sample (non-probability sampling) (Teddlie and Yu 2007) was used to select patients for the first, quantitative phase of the study. This sampling technique meant that only available people could be surveyed. However, the number of participants would depend on the study setting, including the bed occupancy of the oncology ward settings, research timing, and resources. A limitation of one month (from the end of November 2012 till early January 2013) was placed on data collection for the first phase of the current study. Therefore, convenience sampling was chosen to fit the aims of the current study.
A total of 122 questionnaires were distributed to adult oncology patients in the SRCC in Riyadh, of which 100 completed questionnaires were received. The response rate was high at 82%, even though the recruitment period was time-limited due to the need to adhere to the timeframe, which had been set by my sponsors (Saudi Cultural Bureau office in London), at three months to enable completion within a reasonable period.
3.4.5 Quantitative data collection
3.4.5.1 Instrumentation
The European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Group has developed and cross-culturally validated the EORTC IN-PAT-SAT32 questionnaire to assess patients’ perceptions of the quality of hospital-based cancer care (Bredart et al. 2005, Bredart et al. 2007; Arraras 2009). The development of the IN-PATSAT32 was based on existing patient satisfaction questionnaires, as well as interviews with oncology specialists and cancer patients (Bredart et al. 1998). The psychometric properties of this questionnaire have been tested and have been used in different countries (Bredart et al. 1999; Bredart et al. 2003; Arrora et al. 2010; Pishkuhi 2014) and translated into different languages using the EORCT translation guidelines (Cull et al. 2002).
The EORTC IN-PATSAT32 was constructed as comprising eleven multi-item and 3 single-item scales. These include the doctors’ technical skills (items 1–3), interpersonal skills (items 4–6), information provision (items 7–9), availability (items 10, 11) scales; the nurses’ technical skills (items 12–14), interpersonal skills (item 15–17), information provision (items18–20), availability (items 21, 22) scales; the other hospital staff’s interpersonal skills and information provision scale (items 24–26); the exchange of information single-item scale (item 23); the waiting time scale (items27, 28); the hospital access scale (items 29, 30); the comfort single-item scale (item 31); and the general satisfaction single-item scale (item 32) (See Appendix 10 for the IN-PAT SAT32 Questionnaire).
Items are all rated on a five level Likert scale with the category labels ‘poor’, ‘fair’, ‘good’, ‘very good’ and ‘excellent’. This response scale has been proved to have methodological advantages over other types of response scales (Ware and Hays 1988). Additionally, the socio-demographic data were collected for each patient including age, gender, marital status, educational level and place of residency. The choice of this survey instrument was justified because it is a well-validated measure of oncology patient satisfaction in the Western context and still applicable to Saudi Arabia’s healthcare system as this instrument has been used in another dominate Arab country; Morocco (Obtel et al. 2011).
3.4.5.2 Questionnaire distribution
For the first phase of the current study, data was collected through use of the abovementioned EORCT IN-PATSAT32 questionnaire. It took approximately fifteen minutes for each participant to complete it.
The distribution of the questionnaire was an important part in the data collection process. I was aware of the potential of bias in the distribution that could introduce bias into the data collected. Eligibility was based upon the fact that a person was being treated in an oncology setting and that they could understand the questions being administered. The nurse educator coordinating the administration of the questionnaire was careful not to coerce or pressurise potential participants. This was done by making clear that participation was not mandatory and there was no effort to persuade or compel a person to take the questionnaire.
The questionnaires were expected to be completed by the patient by themselves but also with the help of their family or others, if required. This was possibly an issue for those who felt unwell or had poor literacy. The issue of literacy was a potential problem for many older and less educated patients. In practice, there were some participants who needed to receive assistance in order to complete the questionnaire. This may have introduced a level of bias, but as long as the patients gave their views freely to those filling in the questionnaire and they faithfully recorded them, then the possibility of bias was limited.
To further reduce the potential for researcher bias, there was no effort to restrict the questionnaire to any pre-selected group or type of individuals and this limited researcher bias in the selection of participants.
However, there is always some measure of unintentional bias in even the most objective research. The manner in which the data was collected could be unintentionally biased. According to Efron (2010) the sample obtained was through convenience sampling; that is the sample is composed of individuals that are available for the survey. Efron (2010) asserts that such forms of sampling are always biased as they include people whom the researcher chooses based on established criteria that they create on their own. . Often time, such a technique results in oversamples people who have strong opinions and under-sample individuals who do not care much about the topic of the survey. The use of this specific sampling method has caused a degree of self-selection bias. The self-selection bias makes determination of causation more difficult to comprehend. For this particular study, the decision to participate in the study may reflect some inherent bias within the characterization or traits of those participating.
For instance, older patients, because of their cultural expectations may have felt compelled to participate in the study, even though it was made clear to them that participation was voluntary.
There was a concern over confidence in patients answering the questionnaires truthfully as nurses were collecting the questionnaires from them. From a scale of 1-10 with 1 being the lowest confidence and 10 being highest confidence of patient truthfulness, I rate my confidence as being 7. It is possible that patients had not answered the questionnaire truthfully in fear of being scrutinised by the nurse. Then there is the issue of a patient receiving help from family members and this could lead to potential distortions in the collection of data. There was always a possibility that a family member could not record a patients’ response to a questionnaire faithfully. This could introduce a measure of bias into the findings.
There is concern that many participants were not have adequate literacy skills to comprehend and answer the questions. There is also a possibility that family members also did not possess the needed literacy skills to comprehend and answer the questions. This may have led to distorted results as a clear and concise picture quantitatively is not obtained due to a bias that arises from non-comprehension of questionnaire.
The high scoring in the questionnaires could be related to the fact that the nurse educator collected the completed questionnaires. This has been shown in the literature to skew the responses of the patients. When nurses collect data the scoring is usually higher. This limitation in the distribution and collection of data is acknowledged. The completed questionnaires were placed in a sealed envelope by the patients before being handed to the nurse educator. The restricted timeline for the research meant that I was unable to collect the completed questionnaires in any other way.
About eight of the questionnaires were incomplete and there was some missing data. This could also lead to a bias in the data collected. The responses to the questions even in the incomplete questionnaires were accepted and used in the study. There was no need to impute the values, delete a question or to reject a questionnaire from the study since the missing data was not sufficient to distort the findings. This was because the sample size was sufficiently large. The missing data did not affect the coherency of the data.
3.4.5.3 Cultural considerations
It must be acknowledged that the use of a translated questionnaire has the potential to present difficulties. Strauss and Corbin (2008) suggest there are four criteria to consider when using a translated questionnaire: (1) fit, (2) understanding, (3) generality, and (4) control. As IN-PATSAT32 is considered to meet these requirements, the existing Arabic Moroccan version of this questionnaire, first used by Obtel et al. (2012) when assessing Moroccan cancer patient satisfaction, was used. As it had been piloted in Arabic, it was regarded as a validated tool (Serhier et al. 2011) and suitable for use in the current study. Slight adaptations in the Arabic were required due to differences between Moroccan and Saudi Arabia, and EORCT has translation guidelines for forward and backward translation (Cull et al. 2002). Any adaptations for language were undertaken cautiously with the assistance of an expert advisor, Dr. Obtel, who is an oncology doctor.
The questionnaire was reviewed by the Saudi ethics committee chair in the SRCC. Also, the questionnaire was tested to determine language suitability with Arabic speaking university students at the University of Stirling before data collection for the current research was conducted. This process helped to identify any cultural barriers and ensure the language used in the questionnaire was fully understandable to Saudi patients.
3.4.6. Quantitative data analysis
The IN-PATSAT32 data were scored according to the available validated scale module (Bredart et al.2005) (See appendix 11 for the Scoring module). Scores for each of the fourteen subscales of the questionnaire were determined for each patient. All the scores for all items in a particular subscale are summed, and then divided by the number of items in that subscale. The scale scores are then linearly transformed to a 0-100 scale with a high score reflecting a higher level of satisfaction.
The data collected from the questionnaire (INPAT-SAT32) was then entered into a statistical package (SPSS, version 19), for processing and statistical analysis. The statistical analysis resulted in descriptive statistics of the questionnaire items, which are described and presented in chapter four. Information presented includes the percentage of respondents, the means and the standard deviation.
The data from the original Likert scale is also presented, together with that data having been subjected to a linear regression. The original data from the Likert scale presented a range of scores and these are analysed. Linear regression involves identifying and determining the relationships between variables. In the data collected in the original Likert based questionnaire, there were questions related to patients’ satisfaction with their care. The linear regression allows statistical analysis of the relationships between the various variables (that is the individual responses to the Likert based questions). This then allows the researcher to describe the relationships between the variables in the responses to the Likert questionnaire. Such relationships thus help to achieve a description of the samples’ satisfaction with regard to individual issues that are encapsulated in the questions, and in doing so these allowed me to build up (and then evaluate) an overall picture of patient satisfaction among this sample.
3.5 Phase 2: Qualitative method
3.6.1 Qualitative design: Semi-structured interviews
Data was gathered through interviews with the participants selected from those who had answered the questionnaire used in Phase 1 and had agreed to be interviewed. It was also important to test the interview schedule in the initial interviews through a test interview conducted between the researcher and a university colleague (Ritchie and Lewis 2003). Interviews are deemed suitable to explore attitudes and beliefs (Gordon 1975), and they can be structured, unstructured (open), or semi-structured (Mason 2006; Walliman 2005).
Semi-structured interviews were used in the current study for the following reasons: (1) to elicit the participants’ perspectives on what areas were deemed deficient, satisfactory, or excellent regarding the care they had received, or to fill in the gaps that had been highlighted following analysis of the questionnaires; and (2) for complementarity. There are some researchers who argue that the credibility of research is often affected when it is based on semi-structured interviews (Creswell, 1998; Patton 2002), for example, because the meaning or wording of questions may be interpreted differently by the respondents. However, other researchers (Barribal and While 1994; Opie 2004) lend their support to the use of semi-structured interviews. Careful consideration was taken throughout the research process to keep both perspectives in mind. The questions were developed keeping in mind the comprehension level of participants can vary so very layman words were used and omitted any particular jargon. During the test phase of interview testing, the questions were securitized to ensure that a single interpretation is concluded by participants. This means that the participant was able to comprehend what the question is asking of them. This had ensured that the respondent provides an answer that is on target to the question. Semi-structured interview questions in a healthcare setting are not uncommon but for this particular study, there were many factors and concerns that influenced them. One of the major factors kept in mind was the varied literacy rate and comprehension levels of the respondents. Therefore, during the test phase of interviewing, all questions were examined and discussions that took place from the questions were closely monitored to ensure that participants were comprehending the questions asked of them.
3.6.2 Participant recruitment
Participants who responded to the questionnaire during Phase 1 were invited to participate in follow-up interviews. Participation was invited at the conclusion of the quantitative questionnaire by asking patients to indicate if they were interested in a follow-up interview. I contacted those who agreed to interview by telephone to arrange an appointment and obtain verbal consent (see Appendix 8 for the interview consent form). Patient information and contact details were entered into the interview recruitment log to manage the research recruitment process (see Appendix 9 for the interview recruitment log).
3.6.3 Sampling methods
The sampling approach for Phase 2 was based on the results from Phase 1, but also relied on the agreement of the participants to be interviewed. Thus, selection of the sample for the interviews was largely based on convenience sampling. That is, the selection was based on those who were actually most readily accessible when conducting the study (Burns and Grove 2007). Such convenience sampling uses non-probability sampling techniques based upon accessibility and ease of access to participants (Marshal 1996).
Throughout the study, convenience sampling was used because of issues of access and time. These restraints meant that the researcher could only identify a sample based upon those who she could conveniently approach in the oncology ward and those who were willing to participate. The convenience sampling method was also used since participation was based on the patients who had already completed Phase1. That is, only those who had previous access to the questionnaire were included in the sampling.
Of those who completed the quantitative questionnaire, 100 were invited to participate in follow-up, qualitative interviews. Of these, 38 expressed their interest, with 23 subsequently leaving contact details, and one person dropping out because of personal reasons, making a total of 22 participants for the interviews. This is a relatively small sample, but, representative as discussed later in chapter five. It was sufficient to gather rich data so that it became common in the later interviews to be presented with views and experiences similar to those that had already been reported.
3.6.4 The development of the interview schedule
The aim of Phase 2 of the mixed methods study was exploratory in nature, to help gain a deeper understanding of patient satisfaction in the KSA. The interview design was informed by several practical considerations, including a need to ensure each interview took no more than 30-45 minutes to avoid tiring the patients (Rhemtulla and Little 2012). An interview schedule was prepared to elicit the participants’ perceptions of patient satisfaction. The interview schedule included a brief discussion on an outline of issues, a list of topics and subtopics relevant to the research, and the primary research question (Green and Thorogood 2009); the questions were adapted and refined based on the results of Phase 1.
It is important to recognise that researchers should use interview schedules with caution, as they can challenge the exploratory aim of qualitative research (Arthur and Nazroo, 2003). Accordingly, the interview schedule was derived from the quantitative phase by identifying a number of key issues. The areas of interest that were coherent with the research question were selected based on the INPATSAT 32 results. It was anticipated that the broad areas of interest would be evaluated and explored in the interviews, for example, clinical effectiveness and accessibility to health care.
These broad areas were then broken down into more specific and manageable concepts in order to facilitate further exploration. For example, the doctors’ skills, nurses’ skills, information exchange, service organisation/accessibility, and general satisfaction were identified as the specific areas of interest that were essential to be covered during the interviews. This led to a semi-structured interview schedule built around the results from Phase 1, but the actual interview used open-ended questions to allow scope for the patients to present their own views and provide answers in their own words (Bryman 2004). The interview questions in the schedule were checked and approved by my supervisors, ensuring the questions were not leading questions focused towards generating responses that reflected my personal opinions.
Following approval, the English version of the interview schedule was then agreed by my supervisors and prepared for translation to Arabic. As mentioned previously, translation was an important step as there was a need to ensure that the questions and wording were consistent with cultural considerations. It was also important to test the interview schedule in the initial interviews (Ritchie and Lewis 2003). Therefore, in the first couple of interviews, it was possible to assess how well the interview schedule was working according to the types of data that I was generating and whether these data met the study aims. The prepared interview schedule can be found in Appendix 20.
3.6.5 Qualitative data collection
A majority of the interviews conducted were through telephone rather than face-to-face. The use of telephonic interview came about from various reasons. Firstly, there was a need to adhere to a specific timeframe in completing field work for the current study. Also, many of the oncology patients who were discharged after the survey was completed gave rise to difficulties in transport as face-to-face interview meant travelling a great distance. It was also observed that a majority of the participants felt more comfortable with telephonic interviewed. The face-to-face interviewed conducted within the oncology ward provided a great deal of insight into the participants behaviours during the interview which clarified patient satisfaction to a great extent from observing non-verbal gestures and cues.
3.6.5.1 Telephone interviews
Telephone interviews were administered to oncology patients who could not be reached for face-to-face interviews due to distance, or because of the patient’s own preference for a telephone interview. It is noteworthy that problems with recruiting participants for face-to-face interviews (even for practice interviews) are common (Mann and Stewart, 2000). Telephone interviews have been previously used successfully for qualitative semi structured interviews (Bowman et al. 1994; Barriball et al. 1996). However, one advantage of telephone interviewing is that it extends access to participants (Mann and Stewart, 2000).
Telephone interviews are considered to be a credible and robust method, although the researcher is unable to see non-verbal and social cues such as body-language (Novick 2008). This lack of visual cues is considered a minimal loss in the context of the patients under study, as they were all familiar with the issues raised (Opdenakker 2006). Indeed, there are other social cues available in telephone interviews such as voice and intonation (Opdenakker 2006). In addition, the patients seemed more relaxed, reflective and able to freely discuss sensitive topics during telephone interviews (Sturges and Hanrahan 2004; Irvine et al. 2013). For example, participants were very comfortable in discussing their doctor’s attitude towards them and openly spoke of lack of compassion exerted by doctors to their patients. The telephone interviews, arranged over the phone, especially suited the cultural context, where privacy is valued. A total of 20 telephone interviews were conducted.
3.6.5.2 Face-to-face interviews
Face-to-face interviews were conducted with two patients in the oncology ward setting of the SRCC in Riyadh. Use of face-to-face interviews provided a basis for determining changes in patients’ moods and tone and voice inflection with regard to their satisfaction with the dimensions of care offered by the oncology department (Pop et al.2002). The interview process is described in more detail in the following section.
3.6.6 Interview process
Although face-to-face interviews were desirable, in practice, for most patients, it was not possible to agree a mutually convenient time for interviewing in hospital prior to their discharge. This was because most of the patients had been already discharged from the hospital oncology ward and so had returned to their families. In such contexts, they were often not at liberty to speak because of cultural restrictions. Additionally, the majority of patients resided outside of Riyadh, making visiting them post-discharge difficult, not only in terms of distance but also because it was time-consuming and costly.
In a sequential mixed method study, it is important to maintain a short time interval between the first and second phase and this was managed by the use of telephone interviews. This increases the likelihood of aligning the quantitative questionnaire with the interview schedule (Harris and Brown, 2010). A short interval between the phases was therefore chosen in order to maximise patients’ recollections of the underlying reasons behind their responses in the quantitative questionnaire (Cronoholm and Hjalarsson 2011).
Follow-up hospital appointments for these patients were six to eight weeks post-discharge, and this meant they were interviewed between discharge from hospital and their next appointment. There was also a possibility that patients’ conditions might deteriorate over time, which could have made participation at a later date highly unlikely. Accordingly, under the circumstances, in order to extend access to discharged patients and maximise recruitment for the qualitative phase without compromising the quality of the information, telephone interviews were performed with these patients at a mutually convenient time.
Although it was originally planned to record interviews, this was not possible since the ethical committee of the SCCR in Riyadh insisted on a separate patient agreement if audio was to be used. Since interviews were not recorded, this placed substantial emphasis on effective note taking to accurately capture all participants’ responses. Good notes must preserve interview information by providing an accurate account of the verbal responses and dialogue. A potential disadvantage to note taking over tape recording or videotaping is the possible inability to capture all relevant details (Muswazi and Nhamo 2013).
Additionally the writing process can mean long gaps or pauses in the interview plus the interviewer may find it rather challenging to combine concurrent note taking with guiding the conversation (Beebe 2001). Similarly, Muswazi and Nhamo (2013) describe how note taking disrupts the effectiveness of communication between the interviewer and the respondent. Conversely an advantage of note taking is that it can facilitate data analysis since the interviewer may already have already classified the information into appropriate response categories (Burnett et al.1998). To guard against potential problems I undertook practice interviews, with Arabic students at the University of Stirling and note taking before conducting real ones. The first interview was conducted on the 6th of March 2013 and the last one on the 24th April 2013.
Each interview started with introducing myself to the participant as a research student and healthcare professional not associated with their care. Before starting an interview, a brief review of the aims of the study was performed as a reminder to the participant. This served to further highlight to the patients the importance of their participation in order to generate valuable research data, hence help improve the quality of health care in the future. The fact that the study information would be made anonymous and kept strictly confidential was also emphasised at the outset. I tried to make the participant as comfortable as possible by consciously attempting to establish an informal atmosphere and a rapport with the participant. I also reminded the participants of the voluntary nature of taking part in the study and that they could withdraw at any time. I also encouraged them to ask for clarification if they did not fully understand any of the questions. I emphasised that they should not feel embarrassed to refuse to answer any question should they feel uneasy.
A number of areas of concern became evident during the interview process, which initially appeared to affect the openness of the participants’ responses. Anonymity was one of these, since participants were concerned that any negative perspective they voiced might filter back to the health care professionals caring for them, thus affecting any future care that they might receive in the hospital. All participants were therefore assured of anonymity many times. I also sometimes sensed nervousness and hesitation and a tendency towards formality in the way the participants responded to my questions. This was understandable given Saudi culture and the fact that Saudis tend to be reserved and respectful, granting considerable authority to health care workers and holding them in high regard. Moreover, in the KSA, strong family ties and the hierarchical structure within the family unit means women might feel inhibited about criticising people in authority. Indeed, some Saudi women must seek permission from a male guardian before openly communicating their needs and wishes to health care professionals (Walker 2009). It was therefore not surprising that some people initially felt uneasy about describing negative health care experiences or raising concerns and voicing dissatisfaction over their doctors.
I became increasingly sensitive to these potential barriers, and soon learned how to adapt my interview techniques to encourage informality and transparency. In particular, this meant respecting the patients’ own cultural choices, ensuring an informal ethos, and treating them as individuals, in order to minimise stress. Thus, in order to encourage participants to continue talking and elaborate on particular issues of interest, I used verbal prompts such as, ‘tell me more about’, ‘please explain’, and ‘why do you think that?’ I also followed recommendations made by Fontana and Frey (1994) and ensured I was courteous, friendly and pleasant. As the interviews proceeded, participants appeared to become increasingly relaxed and tended to open up more.
During the beginning of some interviews, patients made many positive comments which might have been interpreted as their having considerable satisfaction with their hospital care. However, as the interviews progressed, participants started voicing concerns over their care, making several negative comments and pointing to areas where they thought improvement could be made. This honesty is consistent with an emotional shift as the interview-interviewee relationship evolves and a rapport develops (King and Horrocks 2010). Nevertheless, the extent to which the participants’ culture adversely affected the transparency of the answers they provided remains unknown. There was awareness that culture was a potential factor that needed to be addressed in the discussion. The context of the findings needs to be accounted for when discussing them. It was important to make clear that the participants were from the KSA and what they expressed was based on how its culture influenced their responses. Any findings derived from these responses are therefore in themselves a reflection of these cultural influences. By introducing the issue of culture as a variable in the discussion of the findings ensured that was at the least acknowledged.
Because of my training in communication as a nurse and my professional skills, this led to an awareness of these constraints and limitations and was important when analysing and interpreting the data. I had an understanding of the difficulties and challenges involved for a patient and how this could have influenced their views. My experience as a nurse in KSA was also helpful as it had provided me with an insight into the cultural assumptions of my patients. My training in communication allowed me to interact with people and to an extent allowed me to overcome any cultural barriers. This and an awareness of the influence of culture allowed for a fuller and more complete discussion of the findings. To a certain extent it was a bit difficult to separate roles as a researcher and nurse particularly in terms of developing rapport that maintains the limit of a researcher. Rapport building as a nurse is more focused on building relationships with patients to ensure quality of care and comfort throughout the delivery of healthcare services. However, as a researcher it is essential to only divulge in communication building to the extent that it provides appropriate information to the researcher. Also, as a researcher it is essential to abstain from bias by favouring specific participants over another. As a researcher it was essential to refrain from emotional attachments, this is also true for a nurse but to an extent. Therefore, a middle ground was struck which ensure that participants that I valued their input without becoming too emotionally attached to them.
3.6.7 Qualitative data preparation
Generally, interviews create a large amount of data in audio or textual format (Pope et al. 2000). Whilst translating the transcribed interviews from Arabic to English, problems were encountered. Literal (word-for-word) translation can often be inappropriate and lose the actual meaning behind the original narrative (Rubin and Rubin, 1995). The bias inherent in transcript translation in qualitative research has been extensively discussed in previous publications (Brislin et al. 1973; Rubin and Rubin 1995; Temple 1997).
A noted primary methodological dilemma is to use literal translation, or ‘free’ translation, that changes the wording in order to improve the readability and understanding of direct participant quotes. Two risks of free translation are the potential loss of information about the participant, and the possibility of misinterpreting the meaning of their words (Rubin and Rubin 1995). In an attempt to reduce these risks, I used literal translations as far as possible, but with minor modifications to improve grammar and enhance understanding of their meaning in English. It should be noted the extracts drawn from patients’ interview narratives and presented in chapter 5 should not be regarded as verbatim translations. All extracts represented by translated notes taken during interviews were then imported to NVIVO 10 software, which is an electronic package for qualitative data designed to manage data and assist data organisation (Bazeley and Jackson 2013).
3.6.8 Qualitative data analysis
In qualitative research, there are diverse approaches for analysing qualitative data. However, it is argued that qualitative data analysis should be aligned with the research aims and theoretical framework that underpins the research (Pope and Mays 1995). I chose thematic analysis which allowed the themes that were present in the data to merge both from the quantitative and qualitative was helpful in (Fereday and Muir-Cochrane 2006). Thematic analysis is defined as a search for themes that emerge as being important to the description of the phenomenon (Daly et al. 1997). Thematic analysis helps to describe and organise the content of interviews through coding and categorisation of data into themes and sub-themes (Creswell 1998). By taking a hybrid approach it is possible to facilitate both inductive and deductive development of coding, which means a combination of the data-driven inductive approach (Boyatzis 1998) and the deductive a priori code template, as described in the next section (Crabtree and Miller 1999). Accordingly, it fits the research questions by allowing the phenomenon of patient satisfaction to be fundamental to the deductive thematic analysis, whilst also allowing for themes to emerge from the data by inductive coding. Additionally, it is aligned with the mixed methods framework of the current study, as connecting theory and data by moving back and forth between theories and data (both quantitative and qualitative) is an essential part of creating a theoretical understanding (Morgan 2007).
3.6.8.1 Thematic analysis using coding
Six major stages are identified by Fereday and Muir-Cochrane (2006) in the use of a process thematic analysis: (1) development of the coding manual; (2) testing for coding reliability; (3) identifying the preliminary themes which have emerged from the data; (4) applying templates of codes and additional coding; (5) connecting the codes and identifying themes; and (6) corroborating the identified themes by the process of confirming the findings. The coding process was carried out based on these stages as described next.
Stage1: Developing the coding manual
A coding manual is important because it helps a researcher to clearly recognise the textual data from the transcribed interviews (Crabtree and Miller 1999). In addition, it enables the researcher to divide the textual data into segments, to label each identified segment, and to further assess the developed interview segments for evidence of reoccurring themes (Miles and Huberman 1994; Janesick 2003).
I developed the coding manual based on the research questions and the results from Phase 1 then compared it to the qualitative data received in phase 2. For example, coding was categorised into three components. The codes were identified as those factors that were influential in determining a patient’s level of satisfaction with their care based upon the Donabedian (1980) quality of care model. The coding was based on the findings and the themes that emerged were somewhat different from the initial expectations. This is a common feature of research and it is an expected part of the research process. With regard to clinical effectiveness the analysis clarified the measure of clinical effectiveness for the purpose of the study.
The themes that emerged were (1) clinical effectiveness, (2) structure of care (accessibility to health care), and (3) outcomes of care (patient satisfaction). Within the domain of the three main codes, five sub-codes were identified: (1) doctor skills as a process of care, (2) nurse skills as process, (3) information exchange as process, (4) service organisation as structure of care, and (5) general patient satisfaction as an outcome of care.
However, it is argued that a credible code must capture the qualitative richness of the phenomena (Boyatiz 1998). Therefore, codes were identified by label, definition of what the theme concerns, and a description of when the themes occurred. Table 1 provides an example of the coding manual that was developed.
Table 1 - Example of a Priori Coding Developed from Templates of Codes Related to Patient Satisfaction
Code 1 | Definition | Description |
Label: Process of Care | Clinical effectiveness | doctors’/nurses’ interpersonal skills technical skills information provision availability information exchange |
Code 2 | Definition | Description |
Label: Structure of Care | Accessibility to health care service organisation | hospital environment access to department medical personnel attitudes lab services admission services |
Code 3 | Definition | Description |
Label: Outcome of Care | Patient satisfaction | general patient satisfaction during hospital stay |
In applying a NVIVO computer-assisted method in qualitative data analysis, I coded the interview data based on initial key topics in the coding manual. NVIVO was used because it is easy to use and it is easy to import data from the MS-Word processing package (Morrison and Moir 1998; Richards 1999). Further use of NVIVO makes it possible to determine coding stripes from the margins of the document, an aspect that made it possible to determine which code had been used at which point.
However, computer-based data analysis and coding were implemented with full knowledge of the limitations of computer-assisted coding methods (Bourdon 2002). For example, there are concerns that use of computer-assisted methods may result in ‘guiding’ the researcher only in a particular direction. This disadvantage occurs due to the capacity of computer-assisted methods to create a sense of detachment from the actual data (Bazeley and Jackson 2013). Despite these limitations and critiques, computer-assisted methods promote accuracy and transparency in the data organisation processes.
Within the NVIVO software, the creation of codes is achieved through use of free nodes present in the navigation view window or by using the ‘create and analyse’ tab that is located in the ribbon of commands (Richards 2009). For example, interview data related to clinical effectiveness generated 32 free nodes. If a new code was identified, I re-read the annotated extracts from interviews to ensure the new codes were appropriate to textual data. Thus, I repeatedly reviewed and refined the coding manual before I generated the final coding framework.
Stage 2: Testing codes reliability
In order to achieve coding reliability, it is recommended that two or more researchers individually code an interview transcript, rather than relying on single researcher (Stewart et al. 2007). Therefore, I checked the coding framework with my supervisors and compared it with the interview data. Overall, agreement of coding was high, and the few minor issues were discussed and resolved before proceeding to the actual analysis.
Stage 3: Summarising data and identifying initial themes
Summarising the data was achieved through repeatedly reading and re-reading the raw data and outlining key points in relation to the questions I asked during interviews. Table 2 demonstrates the process of summarising data.
Table 2 - Example of the Process of Summarising Data
Research Question | Summary of Responses |
Doctor communication aspects | listening, psychological support, kindness, information about illness progress, understanding and responsiveness were important aspects of communication to participants |
Stage 4: Applying template of codes and additional coding
The template of codes was applied to facilitate the template analytic technique, as suggested by (Crabtree and Miller 1999). The coding manual was used to ensure systemic application and to identify the important sections in the text. All the codes from the coding manual were entered into the NVIVO software as free nodes. From this basic structure, the free nodes were organised and categorised according to four groups of data: (1) clinical effectiveness of doctors, (2) clinical effectiveness of nurses, (3) accessibility to health care, and (4) patient satisfaction as outcome of care. Table 3 demonstrates the method of coding three data sets by applying codes from the coding manual.
Table 3 - Deductive Coding Using Codes From The Coding Manual
Name of theory-driven code | Care Assessment Based Model: (Donabedian 1982) |
Explanation of Code | process of care (clinical effectiveness of doctors and nurses), structure of care (accessibility), outcomes of care (patient satisfaction) |
Clinical Effectiveness (Doctors’ Skills ) | psychological support, availability, and information regarding illness prognosis |
Clinical Effectiveness (Nurses’ Skills ) | caring, technical skills, patient centred care |
Accessibility of Health Care (Service Organisation) | friendly hospital environment preferred, waiting times for admission needs to be considered |
Outcome of care (general satisfaction) | Generally, patients were satisfied with care while simultaneously having concerns regarding provided care |
Data analysis was not only guided by the coding manual, but also involved inductive coding from annotated extracts that identified new themes (Boyatzis 1998). For example, the concept of power dynamics of doctors that affect patient satisfaction emerged from data during the coding of the clinical effectiveness (doctor skills). An example of this is provided in Table 4.
Table 4 - Example of Inductive Coding from Data
Name of data driven code | power dynamic in doctor communication |
Explanation of code | the perception of doctors as ultimate figures of authority over health in the KSA |
Perception of doctors | perceived as too busy or rushed, unapproachable and as failing to consider psychological status of patient |
Stage 5: Connecting the codes and identifying themes
The process of connecting codes is critical for discovering themes which identify a pattern in the data to describe the observations and then interpret features of the phenomena (Boyatzis 1998; Crabtree and Miller 1999). By connecting similar free nodes, themes were identified and similarities and differences between sets of data were found at this stage, which indicated areas of relevance to the research questions. Additionally, themes started to cluster within the differences identified between the views of participants regarding varying situations. For example, Table 5 shows the process of connecting the codes and identifying themes.
Table 5 - The Process of Connecting the Codes and Identifying Themes
Clinical Effectiveness (Doctors/Nurses) | Factors related to doctor skills: Psychological support by doctors Information provision about illness | Factor related to nurses skills Time devoted by nurses Nurses’ language barriers Psychological support provided by nurses |
Accessibility | Impact of settings (single versus shared room) on patient satisfaction Delay in admission services affects patient satisfaction | |
General Satisfaction | Patients are generally satisfied with provided care | |
Contextual Factors | Power dynamic in doctor-patient communication Multicultural environment (effects of nurses) Role of religion in affecting patient satisfaction Role of family in affecting patient satisfaction | |
Stage 6: Corroborating and legitimating coded themes
In this final stage, it was important to confirm the findings by ensuring that the themes identified were representative of the original data (Crabtree and Miller 1999; Fereday and Muir-Cochrane 2006). Before the analysis moved to the interpretative stage, in which the themes were connected to the explanatory framework, the clustered themes that were identified from the previous stage were reviewed in order to check if they captured key aspects of the phenomena. Also, re-reading the text from original extracts helped to illuminate agreements and disagreements in views between segments of data. Further, the analysis tools in NVIVO, such as queries, text searches, and models, were used to develop the analytical process. Thus, the patterns of meaning, similarities, and differences could be explored and set out. Lastly, core themes that captured the phenomena of patient satisfaction in an oncology ward setting in the KSA were identified. The qualitative findings, including all identified core themes that related to the aspects of patient satisfaction as phenomena, are presented in chapter 5.
3.7 Ethical considerations
3.7.1 Informed consent
It was essential that patients understood that participation in the study was voluntary, and that declining to participate did not mean that they would be disadvantaged in any way regarding their health care provision (Parahoo 2006). All willing patients were asked by oncology nurse educator to sign an informed consent form (see Appendix 8), and were provided with an explanation of the study, participant information sheet (see Appendix 7), to enable them to make an informed choice about participation. Informed consent was also required from those patients willing to participate in the follow-up interview. I contacted participants by phone to apprise them of the possibility of the interview and to discuss with them participation issues.
3.7.2 Anonymity and confidentiality
The identity of participants was protected in the current study through complete data anonymity and confidentiality (Polit and Hungler 2001). Patients and their associated results were assigned study identification numbers, and participants’ answers, records, notes of interviews, and completed questionnaires were kept confidential in a locked cabinet during the study. Data was only shared with my PhD supervisors, and participants were not identifiable at any stage.
3.7.3 Data protection
To ensure adherence to legal requirements (Data Protection Act 1998) and ethical guidelines, I ensured data protection by keeping all data in a secured cabinet. Following completion of the current study, these will be stored in the Archive Section of the University of Stirling for ten years.
3.7.4 Cultural and linguistic barriers
Sand et al. (2007) note that it is important that the researcher be fully aware of the barriers that can affect their research, and, where possible, take preventative actions. One important potential barrier in this research was the form of Arabic used in the KSA. All correspondence, including the patient consent form, information sheet, and letter of approval from the University of Stirling, were translated into Arabic, reviewed by the authorities at the SRCC in Riyadh, and the translation was officially verified. This process of approval took some weeks to complete, and was longer than anticipated and had a bearing on the timings of the study.
An important cultural barrier to consider was that some women who are diagnosed with cancer in the KSA may be influenced by the involvement of a male guardian, as discussed previously. To obtain consent from such women (Rashad et al. 2004; Walker 2009) required having to fully explain the study to the male guardian, which could have adversely affected the woman’s decision to participate. The implications of these socio-cultural issues conflicted ethically with, and would be contrary to, the UK guidelines on good clinical research practice (GCRP) (Medical Research Council, 1998). A further problem in this regard was the inconvenience of having to ensure the availability of a suitable male guardian.
3.7.5 Potential distress
Mcllfatrick et al. (2006) point out that non-malfeasance, justice, and respect for human dignity are the guiding principles for interacting with the vulnerable, and that a researcher’s well-developed sense of reflectivity should go some way to mitigate problems arising. For this reason, consideration was given to the health status of patients throughout the study. For example, those who participated in Phase 1 of the study were first judged to be well enough by gatekeepers and checked by the nurse educator and ward staff before being asked to proceed with the interview in Phase 2. I was fortunate in being able to liaise with oncology staff and the attending physician, because this helped to inform my decisions regarding patient vulnerability. I was also vigilant to detect any sign of patient distress becoming apparent during the study participation. Had this happened, I would have immediately considered withdrawing patients to protect them from any exacerbation of their already poor health. In practice, during the conduct of the study, there were no instances of patient distress, and no evidence of any adverse impact of the research on any participant, hence there was no need to consider any withdrawal.
3.7.6 Researcher skills and resources
Appropriate skills for implementing both quantitative and qualitative data collection and analysis were required in the current study, thus I attended a wide range of university courses during my PhD studies. Further training in the use of SPSS software was also undertaken. For the qualitative phase of the current study, I attended the University of Stirling NVIVO training program. Other skills which I developed during the current research years included managing electronic databases and, English being my second language, I tried to improve my academic writing. Workshops in these areas were attended during the course of the current study.
As a native Arab, I had good understanding of potential socio-cultural barriers which might arise during interviews. I was also able to communicate with the patients in their mother tongue as it was convenient and practical. These positive aspects of my skills helped me build a rapport with the patients, and also helped enhance their trust in me and their willingness to share their views. Potential negative aspects were related to my inexperience in conducting formal interviews, although certainly my experience as a nurse had helped develop skills for interviewing patients which would be transferable to the more formal research setting. To overcome any potential difficulties and to address my novice interviewer status, I practised my interview technique through workshops and through guidance and encouragement from my supervisors, from whom I learned techniques for ensuring there was consistent focus on relevant areas of enquiry. Developing an interview schedule also kept me focused.
As I was an oncology nurse prior to beginning my PhD, I was more comfortable in the oncology setting than someone who had no experience in such an environment. This allowed me to interact and communicate with patients very successfully when seeking a sample. It also helped to secure the informed consent of participants and furthermore it allowed me to create an informal and relaxed atmosphere for the interviews. I had previously worked in this setting and this familiarity was helpful in the distribution of questionnaires, which was useful for the collection of reliable data.
However, interacting with cancer patients as a former nurse is different from studying them. In the interviews, it could be argued that I was interacting with them as much in my familiar role as a nurse as I was acting as a detached researcher. This could have led to potential bias in the data collected, although in many respects the model of the fully objective and detached researcher is not sustainable in the context of informal and semi-structured qualitative interviews. Furthermore, despite having previously worked as a nurse and having considerable experience in dealing with cancer patients, it did not help to establish a rapport with a patient. I had to work hard to establish a rapport with the participants, despite my previous experience. In sum, I would argue that my previous experience as an oncology nurse did not harm the validity of the research but contributed to its reliability.
3.8 Chapter summary
This chapter has provided an overview of the research design employed in the current study and a theoretical rationale for its use. The major aim of the study was to assess factors influencing patient satisfaction in an oncology ward in the KSA. Specifically, the study first sought to identify what factors contribute to or hinder adult oncology inpatient satisfaction with care at the SRCC in Riyadh. Second, it explored why and how these certain factors influence adult oncology patient satisfaction.
The study employed a mixed methods approach in the form of an explanatory sequential design to complement the quantitative and qualitative nature of the research aims.
The research was divided into two phases: Phase 1 made use of a quantitative method, which involved conducting a cross-sectional survey of the satisfaction levels of adult oncology inpatients in the SRCC at Riyadh. Phase 2 focused on the qualitative aspects of the study, including the semi-structured interviews that were carried out with adult oncology inpatients who had answered the initial questionnaire.
The chapter also identified patient recruitment issues and data collection methods, including the sampling technique and data analysis used for each phase. It also highlighted the ethical issues behind the current study.
The findings for both phases of this mixed methods study are presented in the following two chapters.
Chapter 4 - Quantitative Results
4.0 Data Presentation and Interpretation of Results
This chapter presents the findings of data collected using a structured questionnaire to assess the satisfaction of cancer patients in an Oncology ward setting. The variables measured against patient satisfaction included: socio-demographic characteristics, clinical effectiveness of doctors and nurses (skills of doctors and nurses, availability and access to information by patients), and accessibility to health care (services and care organisation) by patients.
The chapter begins with the descriptive statistics of patient characteristics followed by exploratory factor analysis (which is used to reduce the number of variables to those that explain the observed variance in the dependent variable). This was followed by multiple binary logistic regression analyses to examine the degree of association between the components and the socio-demographic variables on patients’ overall satisfaction. This chapter concludes with a summary of findings.
4.1 Socio-Demographic Distributions of Respondents and Patient Satisfaction
4.1.1 Demographic Distribution of the Respondents
This section illustrates the distribution of respondents in regards to their gender, age, educational level, marital status, and residency location. The sample consisted of cancer patients from an Oncology ward setting in Riyadh (N=100). In order to simplify data analysis some variables were standardized. Age variable was collapsed into two categories: younger < 45 and older patients > 45. Educational level variable was also classified into two categories: low education represents patients with primary and intermediate educational level. Higher level of education included patients with high school and university degree or more. Table 6 revealed the majority of respondents were female (58%) who fell within the younger age group (52%). Also, a large percentage of them were married (65%), with only 21% single. Most of the respondents had high levels of education (60%) and resided outside of Riyadh (56%).
Table 6 - Distribution of Respondents’ Gender, Age, Education, Marital Status & Home (n=100)
Respondents (%) | |||||
Gender | Male | 42 | |||
Female | 58 | ||||
Total | 100 | ||||
Age | older group | 48 | |||
younger group | 52 | ||||
Total | 100 | ||||
Marital status | Single | 21 | |||
Married | 65 | ||||
Divorced | 4 | ||||
Widowed | 10 | ||||
Total | 100 | ||||
Education | low education (primary, intermediate level) | 40 | |||
high education (high school, university or above) | 60 | ||||
Total | 100 | ||||
Respondents’ residence | Riyadh | 44 | |||
Outside Riyadh | 56 | ||||
Total | 100 | ||||
4.1.2 Patient Satisfaction
In order to capture patients’ overall satisfaction, they were asked to rate the general level of healthcare received during their stay in the Oncology ward. Most patients reported they were generally satisfied (87%) with the healthcare services, while only 13% were less satisfied (See Table 7). To further analyse patients’ overall satisfaction, cross-tabulations using each socio-demographic characteristic were also performed. In Table 8, the results showed respondents who were female (50%), married (58%), highly educated (52%), and resided outside of Riyadh (48%) were more satisfied than respondents who were male (37%), single (16%), lowly educated (35%), and lived in Riyadh (39%), respectively. Still, overall patient satisfaction only slightly differed between the older age group (44%) and younger age group (43%).
Table 7 - Distribution of Respondents Overall Satisfaction (n=100)
Respondents (%) | |||||
Overall Satisfaction | Less satisfied | 13 | |||
Satisfied | 87 | ||||
Total | 100 | ||||
Table 8 - Cross-tabulation of Gender, Age, Marital Status, Education, Home, and Patient Satisfaction
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Age | older group | Count | 4 | 44 | 48 |
% within Age | 8.3% | 91.7% | 100.0% | ||
% within patients overall satisfaction | 30.8% | 50.6% | 48.0% | ||
% of Total | 4.0% | 44.0% | 48.0% | ||
younger group | Count | 9 | 43 | 52 | |
% within Age | 17.3% | 82.7% | 100.0% | ||
% within patients overall satisfaction | 69.2% | 49.4% | 52.0% | ||
% of Total | 9.0% | 43.0% | 52.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Age | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Gender | male | Count | 5 | 37 | 42 |
% within Gender | 11.9% | 88.1% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 42.5% | 42.0% | ||
% of Total | 5.0% | 37.0% | 42.0% | ||
female | Count | 8 | 50 | 58 | |
% within Gender | 13.8% | 86.2% | 100.0% | ||
% within patients overall satisfaction | 61.5% | 57.5% | 58.0% | ||
% of Total | 8.0% | 50.0% | 58.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Gender | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Marital status | single | Count | 5 | 16 | 21 |
% within Marital status | 23.8% | 76.2% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 18.4% | 21.0% | ||
% of Total | 5.0% | 16.0% | 21.0% | ||
married | Count | 7 | 58 | 65 | |
% within Marital status | 10.8% | 89.2% | 100.0% | ||
% within patients overall satisfaction | 53.8% | 66.7% | 65.0% | ||
% of Total | 7.0% | 58.0% | 65.0% | ||
divorced | Count | 0 | 4 | 4 | |
% within Marital status | 0.0% | 100.0% | 100.0% | ||
% within patients overall satisfaction | 0.0% | 4.6% | 4.0% | ||
% of Total | 0.0% | 4.0% | 4.0% | ||
widowed | Count | 1 | 9 | 10 | |
% within Marital status | 10.0% | 90.0% | 100.0% | ||
% within patients overall satisfaction | 7.7% | 10.3% | 10.0% | ||
% of Total | 1.0% | 9.0% | 10.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Marital status | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Education | low education | Count | 5 | 35 | 40 |
%within Education | 12.5% | 87.5% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 40.2% | 40.0% | ||
% of Total | 5.0% | 35.0% | 40.0% | ||
high education | Count | 8 | 52 | 60 | |
%within Education | 13.3% | 86.7% | 100.0% | ||
% within patients overall satisfaction | 61.5% | 59.8% | 60.0% | ||
% of Total | 8.0% | 52.0% | 60.0% | ||
Total | Count | 13 | 87 | 100 | |
%within Education | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
5 | 39 | 5 | 39 | 44 | |
% within Respondents resident | 11.4% | 88.6% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 44.8% | 44.0% | ||
% of Total | 5.0% | 39.0% | 44.0% | ||
Outside Riyadh | Count | 8 | 48 | 56 | |
% within Respondents resident | 14.3% | 85.7% | 100.0% | ||
% within patients overall satisfaction | 61.5% | 55.2% | 56.0% | ||
% of Total | 8.0% | 48.0% | 56.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Respondents resident | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
4.2 Clinical Effectiveness of Doctors and Nurses
The following set of questions were used to capture doctors and nurses effectiveness. The questions under each of these headings were grouped into the following four categories:
Table 9 - Differential Measurement of the Effectiveness of Doctors and Nurses
Clinical Effectiveness of Doctors | Clinical Effectiveness of Nurses |
Technical Skills (Q1-3) | Technical Skills (Q12-14) |
Interpersonal Skills (Q4-6) | Interpersonal Skills (Q15-17) |
Information Provision (Q7-9) | Information Provision (Q18-20) |
Availability (Q10-11) | Availability (Q21-22) |
The respondents’ views on the clinical effectiveness of doctors and nurses are discussed in this section. Overall, these results indicate broad patient satisfaction with the technical and interpersonal skills, information provision, and availability of the doctors and nurses during their hospital stay in an Oncology ward in Riyadh.
4.2.1 Respondents’ View of Doctors Clinical Effectiveness
As shown in Table 10, respondents were most satisfied with the doctor’s medical follow-up (88%) and knowledge of illness (87%) in terms of their technical skills. Patient satisfaction ranged from 84 to 89% and 84 to 85% regarding the doctor’s interpersonal skills and information provision, respectively. Overall, respondents were least satisfied with the availability of doctors. Only 77% of them were pleased with the visitation time and 79% were happy with the frequency of doctor’s visits.
4.2.2 Respondents’ View of Nurses Clinical Effectiveness
Almost all of the respondents were satisfied with the nurse’s physical examination (94%). However, other technical skills (attention to comfort and care handling) only ranged from 81 to 84%, respectively. The majority of patients were satisfied with the nurse’s human quality (89%), but fewer patients were satisfied with their other interpersonal skills (74-78%). In terms of information provision, more respondents expressed satisfaction with the nurse’s information about treatment (82%). Overall, respondents were least satisfied with the availability of nurses representing 75% of satisfaction. Only 73% of respondents were happy with buzzer promptness (See Table 10).
Table 10 - Respondents’ View of Clinical Effectiveness and Service Organisation (n=100 patients)
Satisfied Satisfied | Less Satisfied Less Satisfied | |
Doctor’s Technical Skills Doctor's knowledge of illness | 87% | 13% |
Doctor's medical follow-up | 88% | 12% |
Doctor's attention to problems | 81% | 19% |
Doctor’s Interpersonal Skills Doctor's willingness to listen | 84% | 16% |
Doctor's interest in personality | 84% | 16% |
Doctor's support given | 89% | 11% |
Doctor’s Information Provision Doctor's information about illness | 85% | 15% |
Doctor's information about medical test | 84% | 16% |
Doctor's information about treatment | 84% | 16% |
Doctor’s Availability Doctor's frequency of visits | 79% | 21% |
Doctor's visitation time | 77% | 23% |
Nurse’s Technical Skills Nurse's physical examination | 94% | 6% |
Nurse's care handling | 84% | 16% |
Nurse's attention to comfort | 81% | 19% |
Nurse’s Interpersonal Skills Nurse's interest in personality | 74% | 26% |
Nurse's support given | 78% | 22% |
Nurse's human quality | 89% | 11% |
Nurse’s Information Provision Nurse's information about medical test | 74% | . 26% |
Nurse's information about care | 78% | 22% |
Nurses information about treatment | 82% | 18% |
Nurse’s Availability Nurse's buzzer promptness | 73% | 27% |
Nurse's devoted time | 75% | 25% |
Other Service and Care Organisation | ||
Discharge information provision | 86% | 14% |
Waiting time for medical test | 68% | 32% |
Speed of treatment | 68% | 32% |
Parking | 62% | 38% |
Department Access | 65% | 35% |
Hospital cleanliness | 85% | 15% |
4.3 Other Services and Care Organisation
Respondents were asked to rate other hospital services and care provided by the organization as a whole. The main categories of other services and care organization analysed are listed below.
Table 11 - Differential Measurement of Service and Care Organisation
4.3.1 Respondents’ View of Other Service and Care Organisation
As shown in Table 11 above, the respondents were more satisfied with discharge information provision (86%) and hospital cleanliness (85%). Respondents were less satisfied with the waiting time for medical test (68%), speed of treatment (68%), and department access (65%). Still, only 62% of them were satisfied with parking accessibility to the Oncology ward.
4.4 Factor Analysis of Observed Variables
An exploratory factor analysis was carried out in order to reduce the number of variables to useful factors and to identify the correlation among them. This section highlights the main results of factor analysis, which included descriptive statistics, reliability measurements, correlation matrix, total variance explained; communalities (i.e., proportion of variability of a variable that is explained by the factors); factor loadings (i.e., interpreted as Pearson correlation of an original variable with a factor); and extraction (i.e. variable reduction using principal component analysis)
4.4.1 Descriptive Statistics of Observed Variables
The above percentage results were also evident when calculating the mean of the observed variables. The highest mean indicates the less satisfaction level. In regard to doctors’ clinical effectiveness, respondents were more satisfied with their support (M=1.11, SD=.314) and least satisfied with their visitation time (M=1.23, SD=.423). In regard to nurses’ clinical effectiveness, respondents were more satisfied with their physical examination (M=1.06, SD=.239), but less satisfied with their buzzer promptness (M=1.27, SD=.446), and interest in personality (M=1.26, SD=.441). With respect to other services and organization, respondents were more satisfied with discharge information provision (M=1.14, SD=.349) and hospital cleanliness (M=1.15, SD=.359), but less satisfied with parking (M=1.38, SD=.488), department access (M=1.35, SD=.479), speed of treatment (M=1.32, SD=.469) and waiting time for medical test (M=1.32, SD=.469). (See Table 12).
Table 12 - Descriptive Statistics of Observed Variables
Mean(M) | Std. Deviation(SD) | Analysis N | |
Doctor's knowledge of illness | 1.1300 | .33800 | 100 |
Doctor's medical follow-up | 1.1200 | .32660 | 100 |
Doctor's attention to problems | 1.1900 | .39428 | 100 |
Doctor's willingness to listen | 1.1600 | .36845 | 100 |
Doctor's interest in personality | 1.1600 | .36845 | 100 |
Doctor's support given | 1.1100 | .31447 | 100 |
Doctor's information about illness | 1.1500 | .35887 | 100 |
Doctor's information about medical test | 1.1600 | .36845 | 100 |
Doctor's information about treatment | 1.1600 | .36845 | 100 |
Doctor's frequency of visits | 1.2100 | .40936 | 100 |
Doctor's visitation time | 1.2300 | .42295 | 100 |
Nurse's physical examination | 1.0600 | .23868 | 100 |
Nurse's care handling | 1.1600 | .36845 | 100 |
Nurse's attention to comfort | 1.1900 | .39428 | 100 |
Nurse's interest in personality | 1.2600 | .44084 | 100 |
Nurse's support given | 1.2200 | .41633 | 100 |
Nurse's human quality | 1.1100 | .31447 | 100 |
Nurse's information about medical test | 1.2600 | .44084 | 100 |
Nurse's information about care | 1.2200 | .41633 | 100 |
Nurses information about treatment | 1.1800 | .38612 | 100 |
Nurse's buzzer promptness | 1.2700 | .44620 | 100 |
Nurse's devoted time | 1.2500 | .43519 | 100 |
Information exchange | 1.1700 | .37753 | 100 |
Other staff helpfulness | 1.1600 | .36845 | 100 |
Admission information provision | 1.1900 | .39428 | 100 |
Discharge information provision | 1.1400 | .34874 | 100 |
Waiting time for medical test | 1.3200 | .46883 | 100 |
Speed of treatment | 1.3200 | .46883 | 100 |
Parking | 1.3800 | .48783 | 100 |
Department Access | 1.3500 | .47937 | 100 |
Hospital cleanliness | 1.1500 | .35887 | 100 |
Patients’ overall satisfaction | .8700 | .33800 | 100 |
4.4.2 Reliability Measurements
The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy index should be greater than 0.5 in order to support the use of a factor analysis and ensure that it is satisfactory. Large values for KMO commonly indicate that a factor analysis of the variables is considered a reasonable step to be taken. On the other hand, Bartlett’s sphericity test was used to test the null hypothesis that the population correlation matrix is uncorrelated (Mertler and Vannatta, 2010). Once the observed significance level is 0.0000 it is considered to be small enough to reject the hypothesis. The KMO coefficient was .820, which is close to one and the associated Sig. value of the Bartlett’s test was significant, p <.001; therefore, the null hypothesis is rejected. The results obtained confirm the sample size is adequate for conducting a factor analysis as the relationship between the variables is strong. The variables have some degree of correlation between them making it a rational idea to proceed with a factor analysis. See appendix 12 for KMO test Table1.
4.4.3 Correlation Matrix
A correlation matrix was utilized to further examine the strength, direction, and significance of the relationship between the variables. The strongest positive correlations were between nurse’s information about care and nurse’s information about medical test (r = .79, p <.001); and nurse’s information about treatment and nurse’s information about care (r =.69, p<.001), which were both statistically significant. The weakest positive correlations were between doctor’s information about illness and doctor’s medical follow-up (r =.02, p =.87); and nurse’s human quality and doctor’s information about medical test (r =.02, p =.83), which were not statistically significant. In contrast, the strongest negative correlations were between patients’ overall satisfaction and doctor’s support given (r = -5.29, p<.001) and patients’ overall satisfaction and nurse’s physical examination (r= -5.28, p<.001), which were statistically significant. The weakest negative correlations were between nurse’s human quality and doctor’s support given (r = -.02, p = .83) and patients’ overall satisfaction and speed of treatment (r = -1.81, p=.07), which were not statistically significant.
4.4.4 Total Variance Explained
The Total Variance Explained provided the eigenvalues of any contributing components and the percent of variance explained by the each component. A total of eight components were retained because they had eigenvalues which exceeded 1, as shown in appendix 13. After rotation, Component 1 accounted for only 12.39% of the total variance explained by the original variables, while Component 8 only accounted for 6.41%.
4.4.5 Communalities
Communalities show how much of the variance in the variables has been accounted for by the extracted factors. High communalities indicate a more reliable factor analysis. Communalities results shown in appendix 14 revealed nurse’s information about medical test explained 82.7% of variance, followed by other staff helpfulness (80.6%), nurse’s information about care (79.5%) and doctor’s information about illness (79.4%). Only three variables (doctor’s knowledge of illness, nurse’s buzzer promptness, and doctor’s willingness to listen) fell below the recommended .60.
4.4.6 Factor Loadings
Factor loadings (see appendix 15) illustrates how variables were loaded into components after rotation based on their coefficient size. An assessment of component loadings was necessary in order to label each component. The variable with the highest loading was hospital cleanliness (.825), followed by doctor’s information about illness (.818) and nurse’s information about care (.795).
4.4.7 Extraction
Principal component analysis was conducted utilizing a varimax rotation. The analysis retained the eight components. Table 13 provides the assigned names given to each component based on the highest factor loadings. The first component comprises items 12, 13,17,21,22 named Nurse Skills. Second component, includes items 18-20 named Nurse Information provision. Third component contains items 2, 4, 9 named Doctor Skills. The fourth component includes items 23, 24 named Staff helpfulness. The fifth component comprises items 27, 28 named Promptness of and accessibility to health care. The sixth component includes items 10 and 31 named doctor support and hospital environment. The seventh component contains items 7, 11 named doctor information provision and availability. The last eighth component comprises items 25, 26 named staff information provision.
Table 13 - Component Loadings and Eigenvalue by Varimax rotation
Factor name Items loaded in the factor | Factor Loading | Eigenvalue | % Variance | |||
Component 1 (FAC1_2): Nurse Skills | 3.96 | 12.39 | ||||
Nurse’s devoted time | .757 | |||||
21 Nurse’s buzzer promptness | .664 | |||||
12 Nurse’s physical examination | .648 | |||||
17 Nurse’s human quality | .641 | |||||
13 Nurse’s care handling | .641 | |||||
Component 2 (FAC2_2): Nurse Information Provision | 3.38 | 10.59 | ||||
Nurse’s info about care | .795 | |||||
Nurse’s info about medical test | .781 | |||||
Nurse’s info about treatment | .724 | |||||
Component 3 (FAC3_2): Doctor Skills | 3.02 | 9.46 | ||||
Doctor’s medical follow-up | .689 | |||||
Doctor’s willingness to listen | .598 | |||||
Doctor’s info about treatment | .580 | |||||
Component 4 (FAC4_2): Staff Helpfulness | 2.58 | 8.07 | ||||
Other staff helpfulness | .762 | |||||
Information exchange | .733 | |||||
Component 5 (FAC5_2): Promptness of and Accessibility to Healthcare | 2.53 | 7.91 | ||||
Speed of treatment | .773 | |||||
Waiting time for medical test | .662 | |||||
Parking | .629 | |||||
Component 6 (FAC6_2): Hospital Environment and Doctor Support | 2.50 | 7.84 | ||||
Hospital cleanliness | .825 | |||||
Doctor’s frequency of visits | .652 | |||||
Component 7 (FAC7_2): Doctor Information Provision and Availability | 2.43 | 7.60 | ||||
Doctor’s info about illness | .818 | |||||
Doctor’s visitation time | .587 | |||||
Component 8 (FAC8_2): Staff Information Provision | 2.05 | 6.41 | ||||
Discharge info provision | .739 | |||||
Admission info provision | .711 |
4.5 Binary Logistic Regression
Using the resulting factor scores from the factor analysis and the socio-demographic variables, four binary logistic regressions were performed to evaluate the degree of association in these determinants on patients’ overall satisfaction. The findings are presented in the subsequent sections.
4.5.1 Doctor’s Clinical Effectiveness and Patients’ Overall Satisfaction
For this analysis, the independent variables were Doctor Skills (FAC3_2), and Doctor Information Provision (FAC7_2) and dependent variable was overall satisfaction. Model fit statistic shown in appendix 16 Table 1 indicates a fairly good-fitting model -2 Log Likelihood = 58.427. The two components, Doctor Skills and Doctor Information Provision and Availability, accounted for nearly 32% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 11.309 and its associated Sig. value was not statistically significant, p = .13. Appendix 16 Table 2 presented the classification results, which indicated the model correctly classified 89.0% of cases.
The summary of model variables displayed in Table 14 revealed the odds ratios; however, the Wald statistics for one component (Doctor technical and interpersonal Skills) was not significant, p = .16. Therefore, the null hypothesis was retained for this component.
Table 14 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | Doctor technical & interpersonal skills FAC3_2 | -.417 | .295 | 1.995 | 1 | .158 | .659 | .370 | 1.175 |
Doctor information provision FAC7_2 | -1.163 | .306 | 14.489 | 1 | .000 | .312 | .172 | .569 | |
Constant | 2.417 | .414 | 34.092 | 1 | .000 | 11.208 | |||
a. Variable(s) entered on step 1: FAC3_2, FAC7_2. | |||||||||
The logistic regression coefficients give the change in log odds of the outcome based on a one unit increase in the variable. For every one unit change in Doctor Information Provision and Availability, the log odds of overall satisfaction increases by 0.312, as seen in Table 14 above. This was the only component that significantly contributed to the model, p<.001.
4.5.2 Nurse’s Clinical Effectiveness and Patients’ Overall Satisfaction
For this analysis, the independent variables were Nurse Interpersonal and Technical Skills (FAC1_2) and Nurse Information Provision (FAC2_2), and the dependent variable was overall satisfaction. Model fit statistic shown in appendix 17 Table1 indicates a fairly good-fitting model -2 Log Likelihood = 54.396. The two components, Nurse Interpersonal and Technical Skills, and Nurse Information Provision, accounted for 38% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 6.940 and its associated Sig. value was not statistically significant, p = .44. As shown in appendix 17 Table2, the results of the classification table revealed the model correctly classified 90% of cases.
The summary of model variables displayed in Table 15 revealed the odds ratios; however, the Wald statistics for one component (Nurse Information Provision) was not significant, p = .54. Therefore, the null hypothesis was retained.
Table 15 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | Nurse interpersonal & Technical Skills FAC1_2 | -1.283 | .319 | 16.165 | 1 | .000 | .277 | .148 | .518 |
Nurse information Provision FAC2_2 | -.201 | .328 | .375 | 1 | .540 | .818 | .430 | 1.555 | |
Constant | 2.455 | .423 | 33.747 | 1 | .000 | 11.646 | |||
a. Variable(s) entered on step 1: FAC1_2, FAC2_2. | |||||||||
The logistic regression coefficients give the change in the log odds of the outcome based on a one unit increase in the variable. For every one unit change in Nurse Interpersonal and Technical Skills, the log odds of overall satisfaction increases by 0.277, as seen in Table 15 above. This was the only component that significantly contributed to the model, p<.001.
4.5.3 Service and Care Organisation and Patients’ Overall Satisfaction
For this analysis, the independent variables were Promptness of and Accessibility to Healthcare (FAC5_2), Staff Information Provision (FAC6_2), Staff Helpfulness (FAC4_2), and Hospital Environment and Doctor Support (FAC8_2), and the dependent variable was overall satisfaction. Model fit statistics shown in appendix 18 Table 1 indicates a fairly good-fit, -2 Log Likelihood = 68.020. The four components, Promptness of and Accessibility to Healthcare, Staff Helpfulness, Hospital Environment and Doctor Support, and Staff Information Provision, accounted for about 16% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 6.307 and its associated Sig. value was not statistically significant, p = .61. As shown in appendix 18 Table 2, the model correctly classified 87% of cases.
The summary of model variables displayed in Table 16 provided the odds ratios; however, the Wald statistics for three components (Staff Helpfulness, Promptness of and Accessibility to Healthcare, and Staff Information Provision) were not significant (p>.05). Therefore, the null hypothesis was retained for these components.
Table 16 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | Staff Helpfulness FAC4_2 | -.163 | .263 | .381 | 1 | .537 | .850 | .507 | 1.424 |
Promptness &accessibility to Healthcare FAC5_2 | -.361 | .307 | 1.379 | 1 | .240 | .697 | .382 | 1.273 | |
Hospital environment & doctor support FAC6_2 | -.555 | .252 | 4.845 | 1 | .028 | .574 | .350 | .941 | |
Staff Information Provision FAC8_2 | -.428 | .271 | 2.499 | 1 | .114 | .652 | .383 | 1.108 | |
Constant | 2.142 | .352 | 37.031 | 1 | .000 | 8.517 | |||
a. Variable(s) entered on step 1: FAC4_2, FAC5_2, FAC6_2, FAC8_2. | |||||||||
The logistic regression coefficients give the change in the log odds of the outcome based on a one unit increase in the variable. For every one unit change in Hospital Environment and Doctor Support, the log odds of overall satisfaction increases by 0.574 as seen in Table 16 above. This was the only component that significantly contributed to the model, p=.03.
4.5.4 Socio-demographic Characteristics and Patients’ Overall Satisfaction
For this analysis, the independent variables were gender, age, marital status, residence, and education, and the dependent variable was overall satisfaction. Model fit statistic shown in appendix 19 Table1 indicates a poor fitting model, -2 Log Likelihood = 72.798. The five socio-demographic variables accounted for approximately 8% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 5.762 and its associated p value was not statistically significant, p = .67. Appendix 19 Table 2 presented the classification results, which indicated the model correctly classified 87.0% of cases.
The summary of model variables displayed in Table 17 revealed the odds ratios; however, the Wald statistics for the socio-demographic variables (gender, age, marital status, education and residency) were not significant (p>.05). Therefore, the null hypothesis was retained.
Table 17 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | AGE(1) | .595 | .781 | .580 | 1 | .446 | 1.813 | .392 | 8.375 |
Gender(1) | .376 | .680 | .306 | 1 | .580 | 1.457 | .384 | 5.520 | |
M.STATUS | 1.177 | 3 | .759 | ||||||
M.STATUS(1) | -.691 | 1.471 | .221 | 1 | .638 | .501 | .028 | 8.944 | |
M.STATUS(2) | .104 | 1.257 | .007 | 1 | .934 | 1.110 | .094 | 13.039 | |
M.STATUS(3) | 19.397 | 20016.756 | .000 | 1 | .999 | 265484571.007 | .000 | . | |
EDUCATION(1) | .118 | .629 | .035 | 1 | .851 | 1.126 | .328 | 3.865 | |
RESIDENCE(1) | .041 | .640 | .004 | 1 | .949 | 1.042 | .297 | 3.655 | |
Constant | 1.524 | 1.371 | 1.236 | 1 | .266 | 4.590 | |||
a. Variable(s) entered on step 1: AGE, Gender, M.STATUS, EDUCATION, RESIDENCE. | |||||||||
4.6 Summary and Interpretation of the Results
The quality of the data was important in assuring the reliability and validity of the results. The quality of the data was established by selecting a representative sample of participants. The data was collected from participants who were all patients in oncology wards. The data collected was through the adapted EORTC 32 INPATSAT validated, Arabic pilot test and questionnaire. The sample size was evaluated using a KMO test and found to be of an adequate size. The data analysis was carried out in such a way that no data was lost or distorted
Generally, most respondents’ satisfaction level with the services received was very high (87%). These results support previous findings mentioned in the literature review that high scores are usually reported in patient satisfaction surveys. The study showed that females (50%), married (58%), highly educated (60%), and resided outside of Riyadh (56%) were more satisfied with the services received during their stay in the Oncology wards.
The exploratory factor analysis was conducted to determine what, if any, underlying structures existed for 32-items of the EORTC IN-PAT32 questionnaire, and to describe and summarize the relationship between this given set of variables. Principal component analysis identified eight factors and they are as follows: Nurse Interpersonal and Technical Skills (5 items), Nurse Information Provision (3 items), Doctor Skills (3 items), Staff Helpfulness (2 items ), Promptness of and Accessibility to Healthcare (3 items) , Hospital Environment and Doctor Support (2 items) , Doctor Information Provision and Availability (2 items), and Staff Information Provision (2 items). These components enabled relationships between responses of patients with regard to their satisfaction to be analysed and allowed for the measurement of the patient’s level of satisfaction. The identified components may assist future research on patient satisfaction in a KSA oncology ward settings.
Binary logistic regression analyses were performed to determine which component loadings and socio-demographic characteristics were significant contributors to patients’ satisfaction. Regression analysis indicated that the factors that were important for overall patient satisfaction were: 1) Doctor Information Provision and Availability, 2) Nurse’s Interpersonal and Technical Skills, 3) Hospital Environment and Doctor Support However, none of the socio-demographic variables were important for overall patient satisfaction
Further exploration into why patients seemed generally satisfied with the care and services provided was necessary. In order to gain deeper insight and understanding, semi-structured interview questions were developed based on the resulting component loadings from the factor analysis. The integration at this intersection of phase 1 quantitative analysis and phase 2 qualitative semi structured interviews was designed to collect high quality data on patient satisfaction.
A discussion of the findings presented here, along with those from Phase 2 (chapter 5), is then provided in chapter 6, where the complementarity of the quantitative and qualitative data is shown. The process of integrating the findings on patient satisfaction in oncology ward settings which was collected from both phases is thoroughly detailed in chapter 6. The implications of the findings and considerations for practice and future research are also considered in chapter 6.
Chapter 5 - Qualitative Findings
5.1 Introduction
In this chapter, the findings from Phase 2 are presented. The organisation of this chapter compiled in order to produce information that will help in answering the research question of the current study; what factors contribute to or hinders patient satisfaction with care in oncology wards in the SRCC? The chapter is organised thematically based on themes that emerged during the interviewing process of the participants. The chapter begins with a summary of socio-demographic characteristics of the respondents which provides insights into the demographic trends of the respondents from which data on patient satisfaction is drawn. The remaining sections of the chapter (5.3.1-5.3.4) categorise the findings of the interview data using themes based on the results obtained from the interviews. These themes are considered as factors which impact patient satisfaction.
Each of the subsections under section 5.3 provide an in-depth understanding of interpersonal aspects of care and accessibility of health care as influential factors that formulate adult oncology patients’ perception of their satisfaction. The findings within these subsections aided in fulfilling the aims of the current study.
To further achieve the aims of the current study, each key theme is presented separately, with relevant examples from the translated interview extracts. These interview extracts were selected based on the coding process and also to represent the wide range of participants’ views. Commentary is provided to link these findings with the literature, where appropriate, and also to highlight any similarities and differences between participants’ responses. The chapter concludes with a summary of the key findings from this second phase of the study.
5.2 Socio-demographic patient characteristics
In Table 1, the socio-demographic details of the participants, outlining their age, gender, education level, marital status and place of residence are presented. It should be noted that there were a high number of young people participating in the study. This high proportion of younger people (<45 years) was due to the largely self-selecting aspect of this part of the research, since the choice of interviews was based on those who volunteered. This may have made the sample unrepresentative of the general target population, since the average median age of the diagnosis of cancer for a man was 58 years of age and 51 for women, in 2010 ( Saudi Cancer Registry 2010). While the current study portrays an age for a man as 46-55 years old or 66-75 years old and for women a median age of 36-45 years olds. The current study’s sample is not reflective of cancer incidence/prevalence in KSA but is a mere reflection of the participants that had volunteered to take part in the study.
Table 1 - Patient socio-demographic characteristics
Age | Gender | Education | Marital status | Residency |
36-45Y | Female | High school | Married | Riyadh |
46-55Y | Female | Primary | Married | Riyadh |
36-45Y | Female | High school | Married | Riyadh |
26-35Y | Female | University | Married | Outside Riyadh |
36-45Y | Female | High School | Divorced | Riyadh |
36-45Y | Male | Intermediate | Married | Outside Riyadh |
18-25Y | Female | Intermediate | Single | Outside Riyadh |
26-35Y | Female | High School | Married | Outside Riyadh |
36-45Y | Female | Illiterate | Married | Outside Riyadh |
36-45Y | Female | High School | Married | Outside Riyadh |
66-75Y | Male | Primary | Married | Riyadh |
46-55Y | Female | Primary | Widowed | Riyadh |
46-55Y | Female | University | Married | Riyadh |
56-65Y | Female | Intermediate | Widowed | Riyadh |
46-55Y | Male | Intermediate | Married | Riyadh |
46-55Y | Female | Intermediate | Married | Outside Riyadh |
46-55Y | Female | University | Married | Outside Riyadh |
36-45Y | Female | University | Married | Outside Riyadh |
26-35Y | Female | High school | Single | Outside Riyadh |
Above 76Y | Female | Primary | Married | Outside Riyadh |
18-25Y | Female | High school | Single | Outside Riyadh |
36-45Y | Female | University | Married | Outside Riyadh |
Based on Table 1, of the 22 participants only two were male. Both of whom were married and resided in Riyadh. However, of the two male participants, one aged between 66- 75 years had only attained primary education while the other male participant aged 45- 55 years old attained intermediate education. The remaining 20 participants were females of varied age, marital status, and education level. The median age of females within the sample was 36-45 years old. Of the female participants 13 were married, 3 were single, 2 were widowed and one was divorced. A majority of the female participants resided outside of Riyadh (11) while the remaining (7) resided in Riyadh. All the female participants except one had attained some level of education. A majority of the participants (7) had attained a high school level education, while the remaining were dispersed with 3, primary, 3 intermediate, and 5 university level education amongst the participating females.
5.3 Key themes emerging from the interview data
The four primary themes identified from interview data are shown in Table 2 and are discussed in extent in the sub-sections.
Table 2 - Themes and Subthemes that Emerged from the Interview Data
Themes | Subthemes |
The doctor-patient relationship | Perception of doctor- patient relationship |
Interpersonal communication | |
The nurse-patient relationship | General perception of nurse-patient relationship |
Technical aspects of nurses’ skills | |
Interpersonal aspects of nurses’ skills | |
KSA cancer contextual factors | Perception of cancer |
Power dynamic of KSA Doctor | |
Religious influence | |
Family influence | |
Multi-cultural environment–nurses’ affects | |
Organisational factors : service organisation | Perception of general service organisation |
Accessibility | |
Waiting times for services |
5.3.1 The doctor-patient relationship
The analysis of participants’ descriptions of their interactions with their doctors provides insights into the aspects of the doctor-patient relationship that are especially meaningful to the patient and influence their understanding of their experiences and the satisfaction with the care they receive.
The doctor-patient relationship in KSA is somewhat different to the western model. The family often needs to be consulted concerning the doctor’s disclosure of information to a patient. Doctors are often required to inform a patient’s family of their treatment and health. This means that the doctor-patient relationship is more complex and that a doctor needs to consider the family in their relationship with their patient. Many patients in the KSA are comfortable with this, because of cultural considerations. However, this particular take on non-disclosure has a significant impact on patient satisfaction and restrains the KSA healthcare delivery from becoming patient-centred. This in turn may have a significant impact on the findings of the study. It is possible that since females are not participant in the delivery of their healthcare they will be less satisfied than compared to male patients. However, although male patients are involved in their healthcare and treatment options, they may not be as satisfied as ultimately the decision for treatment and discussion of patient health status is discussed by the patient’s family. The issue of non-disclosure causes patient dissatisfaction due to their experience with having their health information disclosed to people other than themselves and treatment decisions making be left to individuals other than themselves.
Four main factors were identified that represent aspects of interpersonal communication between doctors and their patients:
- Listening: listening to and addressing the patients’ questions and concerns
- Information provision: providing adequate information about the patients’ conditions and treatments
- Motivation: being encouraging and motivating to the patients
- Care and compassion: being caring and compassionate, with attention to the patients’ psychological as well as medical needs.
These aspects are important to the relationship between patient and doctor despite the requirements for non-disclosure. Based on the analysis of the findings, doctors functioning within the KSA healthcare delivery environment are unable to appropriately deliver these interpersonal communications due to the distraught non-disclosure policy that is family centred. There have been attempts by doctors to do so as evident from the analysis of the findings. Non-disclosure in the KSA setting is influenced by cultural norms, religious beliefs, and attitudes of the doctors. For example, female patients need to have a male guardian who makes the ultimate decisions regarding their healthcare, this will include deciding between treatment options. Therefore, patient information is disclosed to the male guardian of the patient which is ultimately against the philosophical and legal context of non-disclosure. However, this necessary for the doctor to do as it conforms to cultural beliefs of KSA.
The following section presents the participants’ general perceptions of the doctor- patient relationship in the oncology ward at the SRCC in Riyadh. In the subsequent sections the four sub-themes are examined in detail.
5.3.1.1 General perceptions of the doctor-patient relationship
The current study produced varied views among participants regarding the doctor-patient relationship experience. Many built their relationship with their patient in a way that was satisfying, although they were dissatisfied with some aspects.
Fourteen of the twenty-two research participants in the study were positive about their experiences of the doctor-patient relationship. They expressed appreciation and gratitude for their doctors’ personal qualities and interpersonal skills, which had clearly contributed to satisfaction with their hospital stay, despite the non-disclosure requirements that were implemented on all patients including the current study’s sample of 22. Those reporting positive experiences described their doctors in terms such as comforting, trustworthy, helpful, kind, co-operative and patient. For example, two participants stated the following:-
They are so patient and obliging, and dealing with them is easy and comfort(able). (Participant 2)
However, eight participants were critical of some aspect of the doctor-patient relationship. They commented that, although the doctors’ medical expertise was of a very high standard, they were lacking in interpersonal skills, including communication skills, kindness, empathy, and compassion. These views may have been in part influenced by the non-disclosure requirements of their families. Families were consulted by the doctor in regards to the patient treatment options and updates. The eight respondents were not involved in the decision making of their treatment. Crucial care options and information was not disclosed appropriately to patients but was left to the families. This lack of non-disclosure causes patients to feel that doctors are not communicating with them properly when it comes to disclosing information that aids the patient in decision making in regards to their health. The following extracts from participants’ narratives illustrate this:
They told me about chemotherapy and sent me to the health educator to explain the cycles and side effects, which was good. But the doctors here didn’t give the whole treatment plan or future plan to clarify things for me more. (Participant 3)
Because many families restrict information disclosure this prohibits doctors from disclosing information to some patients, especially females. Doctors often need to consult patients’ families on providing information or what should be revealed. This can lead many patients to not being fully informed of their treatment. In fact, many patients are not aware of this family request and the restrictions that it places upon doctors’ level of communication with their patient, especially with regard to the disclosure of treatment plans. This may cause some patients, especially females, to believe that their doctors are poor communicators, while in fact they are only conforming to the families’ wishes.
Indeed, there was no indication that doctors were avoiding contact with these patients. However, in some cases the doctors’ communications with their patients were not satisfying experiences. Females and males are treated differently under the non-disclosure arrangements. However, several males, expressed their opinion that doctors have ‘poor communication’ and this suggests that some patients perceive their communications with doctors as being unsatisfactory.
5.3.1.2 Listening skills
Participants reported that they often had questions and concerns about their illness or treatment, which, if not answered, caused great anxiety and stress. It was important to them to have adequate opportunities to ask their doctor questions or discuss their concerns, and to feel comfortable in doing so. The fourteen participants who mostly expressed satisfaction with the doctor-patient relationship all indicated that their doctors were frequently available to them, encouraged them to ask questions, and provided all the information needed to address their concerns, as the following extracts demonstrate:
They made me comfortable enough to share my concerns with them and patiently listened to me. They answered each of my queries and cleared my doubts. (Participant 15)
They have been very kind and patient. They listen to my concerns and give complete attention to what I say … They answer all my questions no matter how foolish my questions might sound. (Participant 9)
These data show that the majority of the participants were experiencing high levels of personal attention from their doctors, providing evidence of optimum listening skills in the hospital, and indicating that the doctors are addressing the concerns and psychological needs of their patients. This was the case with both males and females and suggested that doctors displayed good communication skills despite the limitations imposed upon them by the non-disclosing cultural attitude. Communication involves issues like ‘listening’ which would not be greatly influenced by any non-disclosure requirements.
In contrast, eight participants reported negative experiences of communicating with their doctors, which they perceived as mainly owing to the doctors’ busy routines and limited time for patient conversations. These participants commented that the doctors seemed unwilling to listen to their questions and concerns, or to provide the information being sought. The following extracts demonstrate this, and also highlight the power dynamics implicit in these doctor-patient relationships:
I … didn’t have the courage to stop them or ask them more as they look busy and just talk quickly during rounds. (Participant 5)
This participant’s concerns and emphasis on his/her own lack of courage convey a state of being afraid to engage doctors in conversation, which may or may not be related to the doctors’ actual listening capacity. However, the subsequent observations made by other participants indicate that this listening capacity may be limited, in some cases:
My talk with them is usually very brief and one sided in which all I had to say was ‘yes’ or ‘no’; they tell and I listen. (Participant 6)
The doctors asked me general questions but were never interested in my specific concerns. (Participant 21)
These comments suggest a power dynamic that is downwards directed from doctor to patient, where the doctor is the one in control of the knowledge that the patients need in order to allay their anxiety. The fact that this anxiety is not adequately listened to, and the knowledge is not shared, highlights an unequal balance of power and control in the patient-doctor relationship here. In particular, the repeated reference to ‘fear’ and ‘courage’ demonstrate the distress some participants felt at not being adequately listened to.
These findings indicate that at least some of the oncology doctors treating the participants in the current study did not give the impression that the participants’ concerns are not of interest. Previous research by Jagosh et al. (2011) argues that physician listening has three very important functions: (1) clinical data gathering, (2) healing and therapeutic value, and (3) building the doctor-patient relationship. While it is uncertain from my findings whether or not the doctors were actually listening to the concerns of their patients, what the study does show is that some felt that they were not being heard. As Ansmann et al. (2013) found, a busy hospital work environment and heavy workload may hinder physicians’ ability to adequately support patients and they may feel constrained in communicating with patients because of any non-disclosure arrangements.
5.3.1.3 Information provision
Most participants reported positive experiences of receiving comprehensive information from their doctors, and noted the calming and reassuring effects that these had on them. The following extracts illustrate this:
The doctors listened to my queries and clarified my doubts in detail. They took every step to inform me well at the start of treatment and also provided me with relevant information during the course of treatment. (Participant 16)
I even had some misconceptions about radiology but they clarified the concepts and now I’m not scared of my treatment. (Participant 11)
These statements would indicate that despite any non-disclosure arrangements in many cases doctors are, in fact, listening to patients and offering them information on their treatment. They are able to clarify a patient’s treatments in a general way and in doing so keep patients somewhat informed. These participants’ statements provide a contrast to some of the more negative perceptions of doctors’ listening skills described in the previous section. Of note is the frequent referral of participants to their lack of clarity regarding their illness and treatments. The responses here, however, certainly suggest some doctors’ efforts to alleviate patients’ anxiety regarding the course of their disease and treatment (even if the prognosis itself may not be positive) through adequate information provision.
It did appear that information provision was problematic for some participants; some reported having to wait too long to receive the information they needed. This was at least partly due to the doctors’ busy schedules, and partly due to the hospital protocol arising from policies of the KSA health service, which prevents the nursing staff from providing certain information to patients. As one participant said:
I am waiting longer to get information about results from doctors, while nurses can’t give me this information until the doctors do their round. I sometimes can’t tolerate the nurses saying that they are unsure about my treatment, as they have to wait for the results and for the doctor to read the results and inform me about progress. This process makes me feel more worried and anxious about my stay. (Participant 5)
Even though some data showed a positive trend toward taking patient satisfaction into account, participant responses such as these indicate that organisational factors such as hospital policies or procedures can sometimes adversely affect the experience of patients and have a negative impact on patient well-being (Aljubran, 2010). The following comments highlight this:
It’s worrisome and irritating to wait so long. Especially for cancer patients, it’s even more irritating to wait. I don’t like it when hospital management forget about the psychological state of their patients. (Participant 13)
I had even requested my oncology team twice to come quickly for the referral visit. They didn’t pay any attention and I’m still here waiting for my psychologist session. I feel so dissatisfied and depressed. (Participant 10)
The stark contrast between these perceptions and those of the participants who were satisfied with the quality and timing of the information they had received conveys high variability in the level of information provision among different doctors at the hospital. What is apparent from these extracts is that long waiting times to receive information can substantially increase patients’ stress levels. Addressing this issue is important since studies have shown that psychological distress has an impact on cancer mortality (Hamer et al, 2008). For example those individuals who expressed dissatisfaction with the doctors’ communication skills could be at risk of poorer health outcomes. This would support the view that non-disclosure could be interfering with a patient’s health.
5.3.1.4 Motivation
The data from the interviews support the evidence that the nature, as well as the level of communication between doctor and patient has a significant influence on patient satisfaction and how it is perceived (Mobiereek et al. 1996; Ezubair 2002). It is clear from participants’ statements that doctors potentially play an essential role in raising and maintaining patient morale, by being encouraging and positive about their recovery:
They advise me to keep myself hopeful. They tell me that I can get healthy again and I’ll be able to live a normal life. I’m so determined to get rid of my breast cancer and I’m thankful to my doctors that they have been helping me so much. (Participant 9)
They were supportive in the success of the treatment. They were encouraging and kind. They sounded like they truly wanted me to get well. (Participant 3)
The key elements here are the nurturing of hope, encouragement, and the perception of genuine well-wishing on the doctors’ part. The doctors’ positive attitudes and the nature of patients’ communication with them may reflect, at least in part, the culture of the KSA, in which physicians are traditionally held in high regard and as figures of authority (Mobeireek et al.1996; Younge et al. 1997; Aljubran 2010). However, in contrast to the negative dynamic of power and control, the findings suggest that there were few doctors who were perceived as listening inadequately to their patients’ needs were not viewed favourably by patients. The doctor’s ability to listen is described as deeply appreciated and seen as responsibly used, i.e. for the psychological improvement of the patient. Being in the position of authority means that compared to other members of the health care team, doctors have a greater impact, either positive or negative, on the health and wellbeing of patients. There were mixed views that appeared in the investigated which included that some of the participants expressed being motivated and encouraged by their doctors which is evident from the quotes below, attesting that communication and relationship with doctors is a significant factor in enhancing patients’ psychological well-being;
I myself didn’t want to stay as I felt depressed, but their motivating words helped me and I started being hopeful. Now, I can proudly say that if my doctors hadn’t stayed positive and supportive, I wouldn’t have been able to come out of my illness ever. (Participant 19)
They have inspired me with their attitude and kindness. They are encouraging, it becomes easier to hope for successful treatment … Their supportive words became my strength and here I’m ready to go home with a healthy body and healthy mind. (Participant 13)
However, the current study had also found contrasting views to those above, these especially surfaced when patients were questioned specifically about their relationships with their doctors.
When doctors are encouraging and motivating, this can be perceived as having a positive impact on the progression of the patient’s recovery. As previous research has indicated, doctors’ communication in an oncology setting can affect the level of patient satisfaction and may also influence the patient’s wellbeing and quality of life (Ong et al., 2000; Wildes et al., 2011).
The practice of non-disclosure could, especially for females, lead to them to build their experiences in a negative way and this in turn could impact upon their health outcomes. The implication of the non-disclosure as a cultural attitude could therefore mean that females are more likely to suffer a negative health outcome than males in KSA oncology settings.
Some participants reported that communication with their doctors had been negative, in the sense that their experiences with doctors were not constructed as encouraging or motivating. This is demonstrated by two participants, who explicitly stated how this had disheartened them and weakened their resolve to recover from their illness:
As medical attendants their behaviour has never been motivating or heartening. (Participant 10)
They have a very casual attitude which I don’t appreciate much. They don’t fill the patient with motivation and determination to fight against their illness. (Participant 6)
These positive and negative examples show the impact that the physician’s manner may have on the psychological state and even on the physical well-being of the patient. These examples also reflect on the connection between a healthy body and a positive mind, as ‘hope’ was a key word emerging in positive descriptions of doctors who were seen as motivating. Previous research argues that a patient’s attitude may be positively correlated with doctor behaviours that are perceived as encouraging and motivating, often resulting in positive medical outcomes such as improved adherence to treatment and self-care (Street et al. 2009). By being motivating and encouraging to the patient, doctors’ communication may have a significant impact on the patient’s state of mind, such as lowering anxiety, and thus, may indirectly influence the overall outcome of the illness episode (Ommen et al. 2010). While it has been argued that an awareness of psychological distress is an essential aspect of patient care, oncology doctors are often unwilling to note the distress in patients, and ask questions regarding patients’ psychological health (Cull et al. 1995; Fallowfield et al. 2001).
The interviews provide insights into the overall impact of a trusting and motivational relationship between the doctor and patient on patient satisfaction and well-being, and particularly on the patients’ abilities to cope with and fight their illness. Participants’ comments tend to support the findings of previous studies that have highlighted the association between a trusting doctor-patient relationship and patients coping with their illness, which may result in improved patient outcomes (Epstein and Street 2007; Arora 2008).
In the beginning of all this I was scared to death and every step of my treatment used to frighten me ... But when I talked about this with my doctors, they listened and gave such kind advice and motivation that finally I started to feel calm. (Participant 4)
The doctors were very friendly and took time to build up my confidence. This provided me with the strength to fight (the) suffering caused by the disease and treatment. I felt comfortable in their presence and that brought a lot of positive energy to me to receive the treatment with great hope and confidence. (Participant 16)
The interview data show a strong link between hope and trust, reiterating the notion of a positive power dynamic between doctors and patients, where the doctors are respected figures of authority who are seen as crucial to reassuring and encouraging the patient with whom they have built up a good relationship. Other research similarly indicates that having a trusting relationship with one’s doctor can have a positive impact on the patient’s mind, generating a more hopeful attitude towards the condition and thus aiding the overall mental state and self-care, which ultimately improves the patient’s quality of life (Clever et al. 2008). Trust could become an issue as a result of the non-disclosure by doctors of issues related to the patient’s treatment. However, there are multiple factors involved in patients’ construction of satisfaction, such as listening and if a doctor concentrates on these then any arrangements between the family and doctor about non-disclosure would not impact too negatively upon patients trust.
Exploring further the connection of trust with patients feeling motivated and encouraged by their doctors, it was found that where there was insufficient trust in the doctor’s genuine interest in the patient’s well-being, feelings of hope and encouragement suffered to the detriment of the patient’s emotional state. For example:
Doctors’ change in behaviour or attitude can make the patient feel ‘unwanted’. Depression and hopelessness take over his mind and his hopes to get healthy fade away. Fear, frustration and sadness fill his mind. (Participant 3)
These findings support evidence from other studies regarding the lack of a trusting doctor-patient relationship, which can negatively influence patients’ levels of satisfaction (Stewart 1995; Parker et al. 2003). It is evident from my findings that, if doctors fail to communicate in appropriate ways with patients, the lack of trust and subsequent lack of motivating and encouraging behaviour may adversely impact on the psychological wellbeing of the patient, and potentially on the clinical outcome.
My findings are similar to those of Fogarty et al. (1999) and Ommen et al. (2010), but additionally provide a deeper, more meaningful contribution to the hitherto poorly researched field of patient satisfaction from the perspective of the KSA context. It would also indicate that more disclosure of health information is important to enhance the doctor-patient relationship and this in turn – based on the evidence that good communications improve patients’ well-being (Aljubran, 2010) – would lead to better health outcomes for those being treated in an oncology setting.
5.3.1.5 Care and compassion
The analysis revealed that a further communication aspect that can have a significant influence on patient satisfaction is when doctors show compassion and care. The compassionate behaviour of physicians is defined by Carmel and Glick as ‘strong devotion to the welfare of the patient on two crucial dimensions of patient care: technical and socio-emotional’ (1996, p. 1253). Doctors perceived as caring and compassionate with patients may provide an element of emotional healing, which could be viewed as a determinant of patient satisfaction (Fogarty et al. 1999; Bertakis et al. 1999).
Many of the participants frequently reported experiences associated with compassion and caring exhibited by their doctors, using terms such as tender, understanding, patient, concerned, and reassuring, and indicating a broader definition of care and compassion. For example:
Doctors have been so tender and (re)assuring. (Participant 13)
The doctors were concerned about me and wanted me recover soon. (Participant 15)
Many also directly alluded to the concepts of compassion, or lack of compassion, when discussing the care they had received from doctors. The absence or presence of compassion clearly had an impact on patients’ overall level of satisfaction with their care. These findings evoke the understanding that an important dimension of patient satisfaction is the ability of the doctor to relate to and engage with the patient as an individual or, as highlighted in the 2001 IOM definition of the patient centred approach, to be concerned with the ‘needs, and values [of the patient], and ensure that patient values guide all clinical decisions’ (IOM 2001, p. 40).
The perceived lack of compassion may have been attributable to doctors’ avoiding close engagement with some patients due to the practice of disclosure of certain health information to families rather than patients. Another possible explanation is that expatriate doctors for whom Arabic is a second language experience difficulty verbally expressing care and compassion to Saudi patients. These expatriate doctors may feel in particular constrained about communicating with patients in the context of the requirements regarding the non-disclosure of information to patients.
The findings indicated that some participants had experienced compassion and care from their doctors according to these terms, which in turn helped them to feel more comfortable in discussing their concerns with the doctor; this also made them feel the doctor was truly interested in their recovery. The following extracts illustrate this:
The doctors were understanding about my need for a sitter[1] and sent me a social worker to facilitate that during my stay. (Participant 20)
The doctors were compassionate enough to give me a few minutes (out of) their busy routine and listen to my concerns. (Participant 10)
These extracts convey that compassion and care was shown towards these patients by showing that the doctors understood and responded well to their personal circumstances, paying attention to their concerns and preferences.
In contrast, other participants commented that the doctors showed inadequate compassion in their communication with them and appeared uninterested in their personal well-being. Thus, these patients felt discouraged from asking questions, and this constraint reportedly made it more difficult for them to cope with their illness:
They don’t have time to talk to patients and everything is so routine to them that they don’t have compassion towards the patient. They just ask routine questions and provide general reassurance. I am suffering so much of it without any psychological support from doctors. It is really difficult for me to cope. (Participant 19)
The doctors are not compassionate at all. They just asked a few questions about our illness but never appeared concerned with our psychological state. (Participant 21)
Two main findings emerge in relation to compassion and the doctor-patient relationship. First, there is a link made between compassion and coping (psychologically), with the implication being that an absence of compassion impacts negatively on the ability to cope. Second, the appearance of a lack of concern on the doctors’ part is recurrent within the participants’ narrative. ‘Concern’ is here distinguished from basic communication, the implication being that it is more than just asking questions, rather it requires a ‘patient-centred’ attitude that achieves a balance between meeting the patient’s clinical and psychological needs.
Expatriate doctors for whom Arabic is a second language may be hindered in expressing care and compassion by the language barrier between themselves and Saudi patients. The language barrier may mean that they appear detached from their patients and not appear as empathic, especially as they may also lack cultural sensitivity. The current study’s findings agree with previous research that indicates the positive impact of doctors’ compassion on decreasing the level of anxiety in cancer patients, which in turn increases the level of patient satisfaction and results in improved medical outcomes (Fogarty et al. 1999).
Patients’ satisfaction in an oncology setting was related to the important role that the doctor plays in all aspects of their recovery, and highlighted the need for excellent interpersonal skills in order for them to fulfil this role effectively:
To me, doctors aren’t diagnosticians only but also the ray of hope. Their behaviour, words and facial expressions are important to me, and the means by which I judge the chances of getting well. (Participant 3)
By interpersonal skills I mean the communication skills and compassion. They need to have more kindness and empathy. Here doctors are good — I don’t say they are bad — but in the situation of these skills and characteristics there is a lot lacking. (Participant 18)
A comment from one of the participants summed up the importance of the interpersonal aspects of the doctor-patient role, which appear at times to be disregarded by the medical profession, but which are often the standards by which doctors are judged by patients:
The patients classify doctors on an additional criterion that is ‘behaviour’. The doctor who’s good at his job but isn’t so supportive or caring is designated as a bad doctor, while the doctors are selected by hospitals on the basis of their abilities and experience. (Participant 3)
These findings suggest that it is not only doctors’ medical expertise that is valued but, also their interpersonal communication skills and the level of trust, compassion and ‘felt’ concern that they bring to their relationships with patients. It also suggests a disagreement between what patients value in a doctor and those attributes and values considered by doctors and important to the organisation. Non-disclosure, and language barriers may all interfere with doctor’s expression of care and may make them appear as remote figures, who show ‘detached concern’, rather than empathy. This may be a factor in patients constructing their experiences when interacting with doctors in a negative way.
5.3.2 The nurse-patient relationship
Findings in this theme can broadly be divided into two elements, which interplay to varying degrees, and show varying experiences of the nurse-patient relationship. The first of these is the sub-theme technical competence, relating to nurses’ professional skills at administering medication and other treatment. The second sub-theme is nurses’ perceived level of interpersonal skills, which are defined as encompassing a caring attitude, showing compassion, and being available to respond to patients’ needs. Beginning with an overview of participants’ overall impressions and general perception of the nurse-patient relationship, the following sections outline each of these key areas in turn, analysing their interplay.
5.3.2.1 General perceptions of the nurse-patient relationship
The majority of participants recognised the importance of the nurses’ roles and were appreciative of their help and attitudes. Those reporting positive experiences when describing their relationship with nurses used words such as ‘kindness’, ‘supportiveness’, ‘accuracy’, ‘responsiveness’, ‘trustworthiness’, and ‘understanding’, as the following extracts show:
They are always willing to help us. It’s so inspiring that despite their busy routine they like to wear a kind and reassuring smile on their faces. (Participant 13)
The nursing staff was very dedicated. They provided a great deal of help and support. They attended to each patient with a smile and performed their work diligently. They made my stay comfortable. (Participant 16)
These comments convey the impact of the nurses’ positive interpersonal attitudes (i.e. being kind and reassuring), as well as their professional qualities and competencies (performing their work diligently), on patient satisfaction.
In contrast, a few participants reported that nurses did not have supportive attitudes, and were sometimes too busy for positive communication. The most noteworthy aspects of dissatisfaction related to issues such as inadequate attention to individual patients’ needs and a lack of psychological support:
Generally, nurses are good but need to recognise the psychological status of the patient by allowing more time to spend with cancer patients when asking questions. (Participant 5)
The nursing staff is good but there’s a lot of need for further development. They are not able to adapt to patients of different mind-sets, having a generalised attitude which isn’t sufficient at all. And that’s the reason I’m not really satisfied. (Participant 7)
The findings also indicate that, in order to deliver improvements regarding the nurse-patient relationship, there is a need to address organisational constraints. These include the low number of trained nurses at the hospital, which places a strain on their capacity and/or capability. It seems that there is a need to increase the number of nurses and enhance their efficiency so that they can devote more time to effective communication with their patients, as illustrated by the responses of two participants:-
They are good but they are very busy and there is a real staff shortage. (Participant 1)
The number of nurses is a drawback, as they are limited. Therefore, sometimes I don’t want to bother them to get assistance for the bathroom, so I asked them to teach me how to disconnect the IV plug, and then it was easier for me to help myself. But of course, when I need them they are around and respond well to my calls. (Participant 18)
The last excerpt highlights the awareness that, while nurses’ capacity may be limited, this is not owing to any technical incompetency or lack of care, but is rather an issue of resources. The positive opinions towards the end of the extract indicate that, despite constraints, nurses do make themselves available to help patients with urgent needs. However, some of participants mentioned a lack of psychological support rather than technical assistance as being the key feature that defined their relationship with nurses:
Nurses need to be specifically trained to deal with cancer patients. They should be aware of our psychological state and their attitude should provide confidence to patients as we sometimes have many questions or are worried about the next appointment or discharge. They should welcome questions and comfort us with patience and kindness. (Participant 21)
This extract gives the impression that the nurses did not fulfil their role appropriately and failed to offer psychological support, which is important for a patient-centred approach to nursing. Moreover this participant felt that nurses should focus more on communication and relationship building. Overall, it was apparent that a nurse not having sufficient time to interact and communicate with patients was a determinant of patient satisfaction with the nurse/patient relationship. These findings concur with those of Shattell (2004) and Rachiadia (2009), who indicate that patients want nurses who are approachable, available, empathic and willing to talk with them, as well as nurses who are not rushed because of their workload and responsibilities.
5.3.2.2 Nurses’ technical skills
Having confidence in professionals’ technical competence represents one of the most important underlying indicators of patient satisfaction or dissatisfaction with nursing care (Dowling 2008; Wagner and Bear 2009; Zhao et al. 2009). The findings indicate that patients generally have positive attitudes towards nurses’ technical skills. Most of the participants highlighted the proficiency of nurses’ professional and technical competence, also asserting that such competence helped to build trust between them and the nurses. A recurrent notion that was also seen to be important in the doctor-patient relationship, was “trust” built on patients’ perception of nurses’ expertise:
Nurses are with us all day round. Their technical expertise in preparing accurate drugs, administering them properly at the right pace and constantly watching for any alarming symptoms, are vital for any patient. I am happy that the nursing staff attending to me were all expert in their profession and I did not face any trouble during my stay. (Participant 16)
Their time management and team work impressed me a lot. They were overburdened yet they managed to deliver the correct drug at the correct time to all the patients. They were well organised and very professional in their job. (Participant 17)
The nurses were very professional and have good experience. They took enough care to be accurate with indicated treatment. Whenever they had a doubt they consulted the doctor to be accurate. I am impressed with their competence. (Participant 15)
These comments reveal a high level of satisfaction with the attendant nurses, which in turn had a positive influence on patients’ constructions of their interactions with nurses.
In contrast, some participants had less positive experiences, in particular voicing uncertainty or concerns over the technical expertise of some nurses. There was often an apparent lack of understanding regarding the nature of the chemotherapy treatment being administered and anxiety over the accuracy of its administration. Such concerns could stem from the fact that the ultimate objective of these patients was to cure their cancer and survive the illness, which depends directly upon the technical skills of the nurses supporting them. The following are examples of these experiences; that is, of problems arising from a deficit in nurses’ skills or knowledge:
In my first visit a nurse had almost given me the very strong tablets intended for my neighbouring patient. But fortunately she realised her mistake in time and I threw up the medicine. Since then I keep a keen eye on my medication. (Participant 6)
Medication administration seems the most important technical skill to me. Nurses should consider the medications they control for patients. They work so closely with patients that they are for the most part the ones who capture drug slips made either by the pharmacist or prescribing doctor. Drug handling is important as well. (Participant 6)
Some participants made several constructive suggestions regarding what could be done to improve the relationship between patient and nurse and implying that more could be done to make their experiences more satisfying in an oncology setting. Examples of possible improvements in the patient-nurse include better time management, better explanation of medication administration and, in particular, enhanced skills at inserting intravenous lines. It was also emphasised that nurses should be better trained to ensure the optimal skills in intravenous therapy, as one participant states:
Hate anaesthesia, it makes me feel very uncomfortable. And it feels even worse if the nurses have to try 2 or 3 times to insert the medication. I wish that nurses could learn to do it and get well trained at it so they would be able to do it with one attempt. (Participant 13)
Researchers argue that patients often view optimum nursing care as a combination of practical skills and professional knowledge, which are agreed as fundamental to all nursing practice (Halldorsdottir and Hamrin 1997; Calman 2006; Duff 2013). From a nursing perspective, competence has been defined by ICN (2005, p. 6) as ‘the effective application of a combination of knowledge, skill and judgment demonstrated by an individual in daily practice or job performance’. Specifically, in terms of nursing definitions, competence reflects the following: knowledge, understanding, and judgment; a range of skills, including cognitive, technical, or psychomotor and interpersonal; and a range of interpersonal attributes and attitudes (ICN 2005). This definition describes a fundamental requirement which influences the quality of care of the participants. The findings of the current studythe current study suggest that there is a need to address nursing competencies, especially in relation to medication administration and the insertion of intravenous lines for chemotherapy.
5.3.2.3 Nurses’ interpersonal skills
Participants mentioned several aspect of nurses’ interpersonal skills as significant: 1) being caring, supportive and compassionate; 2) paying attention to the patients’ psychological as well as medical needs; 3) responding appropriately and taking time to listen and understand the patients’ needs; and 4) ensuring they are available whenever patients need them, even when overloaded with work. By embracing all of these, the nurse-patient relationship was seen to have the potential to evolve into a trusting relationship.
5.3.2.4 Care and compassion
Participants generally felt that nurses should be able to understand patients’ needs. Some vital interpersonal skills that were highlighted related to the level of nurses’ supportiveness, care and compassion. A connection was apparent between the levels of care and compassion shown by nurses and the motivation of patients to get better, which, in turn, related to patients’ level of satisfaction with their care:
They spent time talking with me. I found it so lovely and caring and sensitive to my needs, I really appreciate them and their way of dealing and sharing with patients. I see this as very important to cancer patients, to be surrounded by good nurses who are willing to accept and talk and dedicate their time to us. (Participant 8)
They were caring towards me... Their kindness and sympathetic attitude were always encouraging and helped me to cope during my stay, thank God… They always asked me if I had any complaints or if I needed pain medication. Even if I rang them they were quick to respond and provide me with comfort and help during either their day or night shift. (Participant 20)
In contrast, other participants reported negative aspects of their interpersonal relationship with the nurses, including inadequate attention to the individual patient’s needs and a perceived lack of understanding and failure to supply support. There are several possible reasons for this, including the work load of the nurses. The non-disclosure issue may influence nurses’ attitudes to communicating with patients. They may interpret the non-disclosure requirements of some families as meaning that they must avoid their communications with all patients or they may seek to minimise communication to avoid patients, especially female patients from asking questions, which the nurses are prohibited from answering. This will mean that patients build their interactions with nurses as being unsatisfactory.
Some participants also noted that nurses did not always have enough time to give patients adequate attention. This was complicated by the fact that some of the nurses were non-Saudi nationals, for whom Arabic was a second language:
Generally, the nurses are good but need to recognise the patient’s psychological state by allowing more time to spend with cancer patients when asking questions. They should also ask for a translator if the patient can’t understand some points in conversations, such as helping with room transfer from a shared to a single room. (Participant 5)
This again raises the issue of resources of time and cost for translation, specifically, the challenge of expatriate nurses, who potentially do not have adequate capacity to develop trust and good communication with patients. This may also be due to a lack of proper language training, specifically Arabic. Previous research indicates that, without a shared culture and language, it is difficult for expatriate nurses to deliver effective nursing care to Saudis (Al-Shahri 2002; Al-Dossary 2008). The language barrier may lead nurses to appear as detached and remote to the patients. This is contrary to the patients’ expectations of how a nurse should behave and act (Rchaidia et al. 2009). Such barriers will lead to patients construing their experiences with some nurses, as being unsatisfactory.
The finding discussed in this section have shown the importance of nurses being perceived as compassionate and caring by patients, features that have been highlighted in cross-cultural studies. For example, a review by Rchaidia et al. (2009), who investigated cancer patients’ perceptions of the ‘good nurse’, indicates that the personal characteristics of being caring, showing compassion and relating to the patient as a person are fundamental traits, which pertain to both western and eastern cultures. My findings would suggest (as in the case of the doctors) that cultural attitudes and the language barrier may interfere with nurses’ ability to express empathy and care that is expected of them by patients. If nurses are perceived as not acting compassionately and expressing care then they are not acting in ways that a patient can construe as appropriate or satisfying.
5.3.2.5 Availability: ‘Being present’
The findings demonstrate that several participants had a positive attitude towards nurses’ availability and their time management during care provision:
Their time management is commendable. They attended each patient with great competence. They performed their duties… dedicated enough time to each patient. (Participant 15)
However, other participants noted that nurses were sometimes too busy to give patients the attention they needed:
They just need more time to spend with patients as they have a staff shortage and the nurse couldn’t spend time with me when I asked or called in the afternoon... Then they do attend… but they just need to be faster… one nurse who was caring for me had two beds in the room to look after so I always felt too shy to ask her for help with walking or the bathroom as I could see she was busy and couldn’t help me. (Participant 5)
The emphasis was on nurses being present and devoting the appropriate amount of attention predominantly to patients’ physical needs, but also to psychological needs, since the right attitude can make patients feel more comfortable. According to Rchaidia et al. (2009), this state of ‘being present’ both physically and mentally in terms of their openness to patients’ psychological needs, is an important indicator of a good nurse, based on the perceptions of cancer patients.
5.3.3 Contextual factors relevant to cancer in the KSA
The third theme which is contextual factors seen as specific to the context of cancer in the KSA, also emerged as important to patients’ perceptions of treatment and the level of care being provided. The subthemes of the contextual factors that found are: the patient perception of cancer, culturally endorsed power dynamics regarding the doctor-patient relationship, the influence of religion, the role of family, and the effects of a multi-cultural hospital environment. The next section presents findings from the analysis of interview data regarding these subthemes that emerged from the current study. This facilitates identification of key factors relating to the KSA cancer context.
5.3.3.1 Patients’ perceptions of cancer
Patients within the KSA view certain illnesses, such as cancer, as being of greater medical priority than other forms of disease or illness. Therefore, oncology patients believe they are deserving of greater attention from medical staff and require better treatment conditions. The following quotes illustrate this:
Yes, oncology patients must have priority in appointments for labs or x-ray. (Participant 8)
Organisations should learn to treat cancer patients differently to other patients. They should understand that time is of utmost importance in our treatment. Any delay on their part could have a devastating impact. They could help us a lot by improving the pace of functioning. (Participant 1)
These extracts convey some participants’ perceptions that oncology patients should be given priority in accordance with their special requirements. The second extract, in particular, emphasises the urgency with which the need for treatment is perceived, with words such as ‘priority’, ‘delay’, and ‘pace’ in both extracts denoting the importance of timeliness.
Illness, particularly cancer, is perceived in various ways depending on national or regional cultural factors. In the context of the current study, participants’ perceptions that cancer should have priority status in terms of treatment may be drawn from the cultural beliefs of the KSA that cancer is likely to be an imminent death sentence. For example, one participant commented:
I never knew about cancer and its treatment. In my mind it was just one fatal disease and I knew nothing else about it. But when I came here and the tests confirmed that I had cancer, I started believing that I would be dead in few days. (Participant 12)
Similarly, cancer has been found to carry a social stigma worldwide (Goffman 1963; Albrecht et al. 1982; Chapple et al. 2004; Rosman 2004). However, Joffe (2002) has argued that fear of cancer has decreased markedly as medical knowledge and success rates have increased. Nevertheless, the my findings indicate that cancer within the KSA is perceived in ways that go beyond stigma alone; that is, as a fatal disease which can evoke a strong fear of death.
Another factor that has been found in other studies to impact on oncology patients’ satisfaction is the treatment environment (Gotlieb 2000; Ulrich et al. 2004; Rowlands and Noble 2008). Related evidence has emerged in the current study, where patients’ main concern was not being able to have privacy. The following participants emphasised the importance of having a single room, as being in a shared arrangement adversely affected them physically and psychologically:
I feel so shy when I have nausea in a shared room as I can’t tolerate the smells of food during lunch time. That’s why I am so irritated at sharing a room with someone. But if I am in a single room, I feel comfortable and free to request from the nurse that no food should be supplied to my room due to my severe nausea. (Participant 3)
Having a single room is important for me because I feel comfortable when I can sleep and rest with no noise, and can have a quiet place to rest and read the Quran. I prefer to be alone and not to socialise with people during my stay as staying with people increases my worries and fear as other patient have different treatment and stages, which is not always encouraging to me. (Participant 5)
For example, high-quality environments with high levels of support seem to be associated with higher levels of patient satisfaction, especially for the most severely compromised patients (Timko and Moos 1998a). The findings of the current study also demonstrate the importance of a treatment environment that is sensitive to oncology patients’ needs, particularly the need to be able to express the physical symptoms of their illness without fear of shame or embarrassment. Being unable to do so has a negative psychological effect and may even make patients feel uncared for and despondent over whether they will get better, as the extracts illustrate. A central desire was for a private space if they were very ill. These findings indicate that patient preferences are deemed to be an important element in providing patient-centred care, thus influencing the level of cancer patient satisfaction.
As these findings have shown, patients’ perceptions of cancer specifically in the KSA context, and their experience of the treatment environment both contribute to their perception of the treatment they should be receiving, and the quality of actual care they feel they are receiving. The following sections elaborate on the other key contextual factors affecting this perception.
5.3.3.2 The influence of doctor-patient power dynamics
As shown in section 2.5.2.4 in chapter 2 and section 5.3.1 of chapter 5, the doctor-patient relationship in the KSA context is typically mediated by the perception of doctors being powerful figures of authority whose word should be trusted, rather than encouraging dialogue or discussion between doctor and patient for purposes of shared decision-making.
Patients’ perceptions of doctors in the KSA, and the power imbalance that occurs, can be seen as closely related to the conventional role of physicians in KSA culture. Whether or not they are native to the KSA, doctors are considered to be highly respected figures of authority (Elzubier 2002). As one respondent commented:-
The relationship with doctors is important to every patient. We actually give them, after God, the authority over our body and illness, so having a good trusting relationship with my doctors keeps me calm and satisfied. (Participant 9)
Doctors are positioned as the ultimate human authority on health, who, by implication, have the necessary knowledge and skills to administer whatever treatment is best for the patient, and therefore should not be questioned. This view, in turn, lends itself to a top-down power relationship between some patients and their doctors, as the following extracts illustrate:
The doctors were not interested in patients’ mental condition. They took care of treatment and that’s it. We could not feel comfortable enough to express our concerns to them. This has adversely affected the whole situation by making us feel unmotivated. (Participant 19)
In the beginning, I had endless fears and doubts but I wasn’t able to talk about it with my doctors. I had once tried to tell them about it but they shooed me away and since then I never gathered enough courage to communicate openly with them. (Participant 7)
Both of these extracts imply a sense of being intimidated or ‘not comfortable’ with doctors. In particular, the fact that the second participant’s anxiety is not adequately listened to and the necessary knowledge is not shared highlights an unequal balance of power and control in the patient-doctor relationship. Participant seven’s emphasis on (lack of) ‘courage’ suggests a state of feeling intimidated by those who have the power to allay the fears and doubts associated with the illness. The participant’s feelings may stem from the fact that families wish to restrict information, a cultural attitude. This means that patients can feel anxious because they have little or no information on their treatment keeping them in the dark and questioning the treatment options chosen for them. The anxious feeling and the feeling of being shut out of making decisions of their own body leads to their dissatisfaction of the healthcare provided to them. Patients such as participant seven desire to overcome the family restrictions that are placed on them terms of their treatment and giving them the sole right to decide about their healthcare.
In contrast, several patients mentioned feeling very well-informed by doctors, to the extent of feeling they knew whether their illness would be cured or not. Given the strong cultural context at work, this effect can be seen as part of the high regard in which doctors are held in the KSA. As one respondent stated:
The doctors in oncology were so respectful and helpful, they tell me everything about my condition and options for treatment such as surgery, chemo and radiation, also they were honest about prognosis and this was so important for me to know (whether my disease is) curable or not. (Participant 8)
This finding also reflects a cultural shift in doctors’ information provision to patients in the KSA as evident from the experience of the participants in the current study, indicating that they are increasingly providing patients with full details about their condition, such as the prognosis.
As discussed in chapter 2, studies conducted in the KSA and internationally (Al-Ahwal 1998; Tanaka et al. 1999; Al-Amri 2010) provide evidence that patients prefer to have full disclosure of information about their illnesses. In contrast, surveys of physicians in the KSA (Bedikian et al. 1985; Mobeireek et al. 1996) have revealed their preference for discussing patients’ condition and treatment with patients’ close relatives rather than with the patients themselves. More recently, however, there has been growing public awareness of medical issues, as well as ethical pressures, in the KSA that are reportedly driving a change in doctors’ attitudes and behaviour, with full disclosure of diagnosis to the patient rather than their relatives becoming more common (Sokol 2006; Mobeireek et al. 2008; Al-Amri 2010; Aljubran 2010). The current study’s findings support that doctors in the KSA today provide full disclosure of information to oncology patients which implies that it has become a norm, however, if the family has expressly stated that a patient is not to be informed of about their health or treatment doctors do not do so.
Considering these cultural factors, it becomes evident that the perceived power imbalance between doctors and patients can affect patient satisfaction with care either positively or negatively, depending largely on the interpersonal dimension, that is, the capacity and the way in which doctors deliver the relevant information. Some of the participants indicated the ideal power balance they would like to have with doctors, including a preference for an open and trusting relationship in which they could feel comfortable discussing any of their concerns in a sensitive manner. The following extracts illustrate these expectations:
A patient should trust and be able to depend on his doctor. This relationship develops with understanding and interaction. Doctors shouldn’t be the medicine/treatment prescribers but also a counsellor. (Participant 21)
The personal skills of the doctors here need much improvement as they should consider the psychological state of the cancer patient. I want them to deal with me in a kind way and consider that their attitude will affect the patient, like if they didn’t listen or just try to be in hurry during visits. (Participant 7)
This apparent change of attitude where patients wish to build relationships of trust with their doctors and openly verbalise their concerns is surprising in a KSA context. This preference for patient empowerment and advocacy is arguably at variance with cultural norms in the KSA. These patients’ attitudes, and their emphasis on doctors’ ‘kindness’, represent a shift towards the need for a more western and patient-centred approach involving active patient participation in care.
5.3.3.4 The influence of religion
In the current study, a major point to consider was that the religion of Islam is the main aspect shaping the culture of the KSA. Many of the participants indicated that their faith affected their perceptions not only of their disease, but also of the care they received. These findings add to other studies conducted in KSA which have drawn the importance of faith in receiving healthcare, particularly the study conducted by Halligan (2006) who argues that Islam is a contributing influence on patient satisfaction. He highlights the way in which the influence of Islam can be felt in every aspect of patient care. All of the participants in Halligan’s study, who were expatriate nurses, recounted that everything people do is centred on religion, and it is the main way of life. Consequently, Halligan (2006) correlates patients’ attitudes towards their illness with their religion, which is identified as ‘central to the provision of caring’ (Halligan 2006 p1565). The current study adds to the discussion produced by Halligan (2006) as it brings to surface the impact of religion on patient’s assessment of healthcare delivery while Halligan (2006) focused on experiences of nurses.
In the current study, participants indicated that their belief in God was more powerful than medicine. In addition, some of the participants stated that it is their faith and connection with God through prayer that helps to keep their spirits up, as one person stated:
I believe that my disease has been gifted from God as a test to see how I will be patient and deal with this fact; therefore, I accept my destiny of cancer and I will be working hard to deal with recovery by praying first to God to help me and then also to help my doctors to cure my disease in the near future, Inshallah. (Participant 8)
These finding are in line with other research which conveys the positive influence of religion on coping with cancer; specifically, some have argued that cancer patients in Islamic countries have better coping mechanisms than those in other countries (Ezzat et al. 1995; Young et al. 1997; Silbermann and Hassan 2011). The current study uses patients directly as participants and adds to other research which used doctors or nurses to assess the impact on faith as a coping mechanism when dealing with cancer.
The emphasis on the spiritual dimension of coping in illness was also evident through the fact that SRCCs have visiting religious scholars, who are on hand to lend patients moral support and spiritual guidance through their situation, and some of the participants commented on this aspect of their care:
The weekly official visit of a religious scholar was very helpful and motivating for me and other patients. I felt so great during religious scholar visits and really need the hospital to consider his visits to be daily for patients, as this reassured me and helped me a lot in my spiritual condition during the treatment. When I felt lost I wished to see someone who could connect my heart with God so I could find some peace. (Participant 7)
Religious lectures on Islamic affairs are needed to bring positive changes for us as cancer patients. (Participant 12)
These extracts demonstrate the importance placed on spiritual health by these oncology patients, and highlights how a visit by a religious counsellor or a lecturer on religious themes can fulfil the spiritual needs of the patients. This fulfilment is also shown to improve their mood and confidence about their situation, as conveyed through language such as attaining ‘peace’ and ‘positive changes’.
However, other participants presented contrasting views by emphasising their belief that the doctors and nurses were the only ones who could help them:
I believe that they are the only ones who could clear my mind about my situation. (Participant 10)
This extract echoes the other dominant cultural context that is relevant here, that is, the conventional perception of physicians in the KSA, who are seen as highly respected figures of authority (Elzubier 2002).
5.3.3.5 The influence of family
The principal idea of family is fundamental to the provision of care within the KSA. This is further supported by Halligan (2006) and Younge et al. (1997), who argue that the importance of family has a direct impact on the perceived level of care by the patient. This is especially the case with the family’s ability to influence doctors’ disclosure of information to a patient. These researchers describe family involvement as pivotal to the experience of the care being delivered and as a significant factor affecting the emotional, social, and psychological well-being of the patient.
In the context of the current study, family members were viewed as the principal decision-makers who often dictate the care that patients receive, including the extent of the care to be given. For example, participants in the current study recounted both how families help to direct their treatment and also offer vital moral support:
Thank God my family are with me; this helps me bear the after effects of the treatment. (Participant 21)
However, while the patient’s family has significant influence on the care to be provided, patients still look to the medical staff, such as their doctor, for ultimate guidance and explanation of treatment prior to making any decisions. In the following extracts, participants underline the doctors’ involvement in the process of informing family members as well as the patient him/herself:
But my mother wasn’t able to understand and she was very afraid. The doctors calmed her down and assured her that they wouldn’t be doing anything wrong to me. (Participant 13)
They explained all about the treatment to my husband. (Participant 22)
These extracts underline the critical role of the family, in that they are physically present at key diagnostic stages; the implication here is that they are then expected to be involved in subsequent decision-making about treatment. This is in line with other findings that, in developed countries, patients often demand more resources, i.e. medical staff attention, to be available to their family (Given et al. 2001). However, these extracts also emphasise the continuing importance of medical staff not only for informing and reassuring the patient, but also for reassuring all members of the family. Thus, while the family can be a determining factor in terms of care, patients are also aware that professionally trained medical staff are essential in providing clarification and ultimately informing treatment decisions (Given et al. 2001; Ezubair 2002).
However, the influence of family, although fundamental is still bias towards females. As noted before, female patients in KSA need the presence of male guardians which can be their father, husband, or son depending on their marital status. The treatment decisions of female patients fall on the father or brother if she is unmarried, on the husband if married, or on the son if widowed or divorced with children. This contrasts to the role that women have when the patient is male. The treatment decision making, disclosure of information, and advise given by a doctor or nurse in the case of male patient is restricted to the male members of the family. In the case of a male patient, the wife is not the sole decision maker for her husband, the male family members of the patient are the ones who are handed the responsibility of decision making and being the main point of contact for information. This is due to the societal hierarchy framed from cultural beliefs within KSA which is male-centric and male dominated.
5.3.3.6 The influence of the multi-cultural health care environment
The health care environment and its own cultural context play a vital role in patient satisfaction (Rafii et al., 2008). A major cultural factor in terms of the KSA hospital environment, and prevalent in the specific SRCC examined in the current study, is the presence of largely expatriate nursing and medical staff from all over the world (in particular South Africa, India and the Philippines) who are unlikely to speak Arabic (Luna 1998; Al-Dossary 2008). In particular, the expatriate nursing staff were found to affect patient satisfaction in that their difficulties with the Arabic language created some tension in communicating with patients. Many participants noted that they could only express their emotions and needs clearly in Arabic languages, which these nurses were not always able to understand fully. As several participants commented:
Their language is a bit of problem; it would be easier to communicate with them if they were capable of speaking Arabic. (Participant 10)
Communication skills are the most important, for example, being able to talk freely and ask about treatment, but in my opinion the nurses need to understand more of the Arabic language to be able to deal with patients easily. (Participant 5)
Inadequate communication arising from language barriers can be seen as a determinant of these patients’ satisfaction level, frequently causing a loss of rapport with nurses. Accordingly, Arabic-speaking nurses were deemed more likely to provide the optimum psychological support and to be able to meet patients’ medical needs than non-Arabic speakers. Evidence of language barriers in communication between the patient and their nurses has been reported by a number of studies in the KSA owing to these nurses frequently being non-KSA nationals (Al-Shahri 2002; Attalah et al. 2013). As previously mentioned, there is, however, currently a drive towards employing greater numbers of Saudi Arabian nurses or Arabic national nurses as part of the Saudisation process (Al-Malki et al. 2011).
Because of the multi-national mix of personnel, including many non-Saudi doctors, English was the default language being spoken among professionals in the presence of the patient, and this could create a feeling of anxiety in the patients. The following extract illustrates this:
For example, the doctor saw me and requested some tests or radiology; then I asked the nurse, but she said there was no instruction written by doctors, so I felt lost between doctors and nurses because doctors speak English with them in front of me, which is difficult for me to understand – is he requesting something or just talking? That’s why I felt worried and asked a lot if doctors were requesting tests or x-rays. (Participant 5)
In this patient’s case, the language barrier negatively affected the way patient constructed their experiences. The use of English rather than Arabic by the medical staff led the patient to feel excluded from discussions about his/her own health, and created a sense of dissatisfaction with the care they were receiving. The issue of the language barrier here overlapped with the requirement of non-disclosure to the patient, thus compounding the potential problems with establishing a personal relationship between expatriate nurses and Saudi patients.
Personal relationships can only be established when communications are possible. The fact that a nurse and patient only have limited communications mean that a nurse can appear as not engaging with a patient or may appear as being inattentive. The ability of a nurse to establish a relationship is further impacted by the fact that they often have to ensure that they don’t disclose information to a patient at the request of the family which is considered a norm of non-disclosure in the KSA healthcare setting. This may make nurses unwilling to spend time and interact with a patient. The language barrier and non-disclosure means that often the nurse-patient relationship is not a satisfying one for both parties.
Language barriers must be addressed in order to ensure quality trans-cultural nursing, given the high proportion of expatriate, non-Arabic speakers in the KSA (Luna 1998; Al-Shahri 2002). It can be argued that the gap, identified here and in previous studies, between patient needs and the language barriers of expatriate nurses may adversely affect the degree of care provided, thus lowering patient satisfaction levels (Al-Shahri 2002; Ezubair 2002; Al-Dossary 2008).
This section has highlighted the importance of nurses and other medical staff in oncology wards tailoring their care to patients’ needs and providing a more patient-centred approach, as this can significantly affect patient satisfaction levels.
5.3.4 Organisational factors impacting patient care
This section presents the findings from the study that highlights the organisational factors influencing patients’ satisfaction or dissatisfaction. Based on the participants’ responses, three main factors were identified as important aspects of the service organisation which influenced their overall satisfaction levels: (1) accessibility to healthcare (i.e. having full access to the hospital and permission to use all the necessary facilities); (2) general service organisation and (3) waiting times (i.e. that they should be reasonable and that the staff should be supportive of patients while they were awaiting treatment).
Prior to a more detailed examination of each of these factors, patients’ perceptions of the general service organisation are detailed in the next section. This is followed by a presentation of the findings relating to each of the three key organisational factors.
5.3.4.1 Perceptions of general service organisation
Overall, there was a mix of views among the research participants regarding their experiences of the service organisation, with many indicating that, while they were generally happy, there was some dissatisfaction with the operational structure of the facility.
The majority of participants who reported positive feedback on the general service organisation talked about both the medical services and overall service organisation:
The referral system is good here. Labs and other testing services are very good and prompt. I don’t have any problem with them. (Participant 9)
My overall experience with the service organisation during my stay is good. (Participant 4)
In particular, some of the participants emphasised the high level of effectiveness of cancer support services with regard to the non-medical support they received, including that provided by the social workers:
I wish them all the best as this main referral hospital deals with a large number of patients and still manages to have great services available to us, such as a social worker and Saudi cancer society officer, who always support me. (Participant 16)
I have the ability to connect freely to the Internet during my stay, as well as social worker services that let me feel happy and rest assured. Also the way they approach me is friendly and helps me feel supported and satisfied during my hospital stay. (Participant 8)
However, some of the participants reported negative experiences of the organisation of medical services. The following extract illustrates this factor:
I had to wait for a long time to obtain the approval of referrals. My treatment was delayed because of a delay at the lab. Sometimes it was really troublesome to get things done with them. (Participant 19)
The previous extract highlights one of the most problematic issues, as several participants reported long waiting times for referrals, admission and for labs. The waiting time for psychiatric services was also seen as problematic:
Other services like referral took a long time, it took a long time to get appointments and it was very uncomfortable to be seen by psychiatric services after 1 month. Generally, I don’t like this waiting time because I feel more worried and less assured, which sometimes makes me feel unstable and anxious during my stay. (Participant 3)
These findings demonstrate that, while there are positive findings regarding the healthcare services, there may be a need to improve certain aspects of service provision for oncology patients, particularly with regard to waiting times and doctor availability. The following interview excerpts emphasise this point:
It’s worrisome and irritating to wait so long. Especially for cancer patients, it’s even more irritating to wait. I don’t like it when hospital management forget about the psychological state of their patients. (Participant 13)
What is needed is making more doctors available to oncology patients. (Participant 3)
The opinions arising from these excerpts and discussed throughout this section show that there are several organisational policy factors that may be at odds with patients’ preferences for the treatment setting or logistics of care such as referrals that are not seen as fast enough and a shortage of medical staff on oncology wards.
5.4.4.2 Accessibility to health care
Participants in the current study reported positive experiences regarding access:
It was good and I didn’t face any problems with it as it was well arranged. There were always supportive services, for example from the social worker or from the cancer support society. (Participant 20)
The admission process was good, well ordered. I didn’t have problem in waiting for admission or referral; it was perfect during my stay. (Participant 8)
In contrast to these positive experiences, some reported several problems with accessing the hospital and its facilities; the following is an example:
I remember the trouble I had to bear at my first CT scan. Firstly, it was crowded all the time and the personnel didn’t bother to do things quickly. I had to wait for two hours to get it done. According to them, it was a busy day, but I think if it’s better organised or there is a separate clinic for oncology it would benefit us more and improve our experiences. Also, referrals and labs have been working at a poor pace. My referral to an orthopaedist took three months; I was already on pain medication but still looking to see a specialist as soon as possible to get a clearer idea about the knee pain. (Participant 18)
Sometimes I got correct information but most of the time it was very confusing. There is lack of coordination between departments and nobody is in a position to provide all the information. The people here were also unconcerned with the trouble of the patient. (Participant 19)
These negative experiences relate mainly to the slow pace at which care was given, and the lack of coordination in information giving or confusion regarding the information actually provided. Timeliness was closely linked with efficient access to services, and impacted adversely on patients’ satisfaction if it was not present. In addition, patients’ criticism of crowded circumstances also denotes the importance of the hospital environment when accessing it, which the following section explores in further detail.
5.4.4.3 Waiting times for services
Waiting times are one of the indicators that have been found to influence patients’ perceptions of the health care service and lead them to construct their experiences with it as satisfactory. In the current study, the waiting times for services were mainly positively assessed by the participants, as these extracts show:
I had a very good experience with the service of the organisation during my stay. There was well organised admission in a timely manner, and that was excellent. (Participant 16)
I feel so comfortable and like the earlier arrangement, such as getting my blood test earlier before going to the admissions office, which means that I can process my admission after the oncology staff confirmation, so that is very well arranged and organised and then I will just be waiting for doctors to be seen directly and treatment to be started. (Participant 8)
In contrast to these positive experiences, some reported that usually admission took longer and they had to spend time waiting in the emergency room for oncology doctors to decide and agree about admission. If patients book ahead for the admission process, it becomes easier and means that they can reach the doctor easily without a further waiting period. The following extracts demonstrate several patients’ dissatisfaction with admission and referral times:
I have been referred to two different doctors – a psychologist and neurologist – and neither of them have any available appointments; it has been almost a month now. It has been really hard for me to wait for so long. (Participant 11)
My admission had been delayed for 8 days. Isn’t this unfair and troubling? And the reason behind it is the unavailability of beds in oncology wards. I couldn’t be admitted to any other wards in hospital to receive my scheduled treatment. (Participant 6)
By using language such as ‘unfair’, ‘really hard’, and ‘troubling’, these participants display a feeling of neglect that is experienced by patients being left to wait for long periods of time for medical attention and referrals, in some cases to the extent that they need to seek private care. This feeling of neglect can also be seen as connected to patients’ views that cancer is a priority disorder. Similarly, other professionals have argued that inadequate access to KSA cancer services such as the long waiting times negatively affects the level of patient satisfaction with the care provided (Al-Muziani 1998; Al-Sirafy 2009).
In light of this, another important element to assess is the perceived level of supportiveness of the health care personnel during these waiting times. Participants mainly reported positive experiences, emphasising the staff’s supportiveness, helpfulness and willingness to help:
Whomever I interacted with, they were well informed, nice and patient. They always provided us with the correct information about the services. (Participant 17)
They are cooperative and helpful in guiding me if I need help such as fixing an appointment or changing the time of an appointment; they have been very cooperative with this. (Participant 8)
However, others noted less positive impressions of their communication with the medical staff during the time they were waiting to receive medical help:
They are good but CT staff need to be more kind and patient, especially with oncology patients. Lab services are usually crowded and need more organisation to make sure they have enough space to accommodate all the patients and not have them always waiting in corridors for a lab call as it's not helpful for patients to be in crowds with their pain. (Participant 3)
Another thing is the lack of psychological understanding among medical staff. They don’t try to understand the patient’s individual psyche. (Participant 6)
These criticisms indicate that medical staff need to act kinder and provide more supportive care, especially towards oncology patients, and that they sometimes demonstrate an inadequate psychological understanding of their patients’ needs.
As the following extracts also show, reference to crowded space and a lack of proper organisation indicates that participants felt that having adequate coordination within the health care system was important, yet was perceived as currently problematic and impacting on waiting times. This is illustrated by one who stated:
There is lack of coordination between departments and nobody is in a position to provide all the information. For example, my next readmission date was not provided until after discharge as the clerk was unavailable that day, so we had to follow this up with them after discharge and my son had to go back to get it confirmed. (Participant 21)
Another connected the problem of long waiting times with the shortage of nurses and the approachability of available staff noting that:
Here the situation is dependent upon the individual personnel; some of them are willing to help and some aren’t. No, I can’t reach out to all personnel if I need, they don’t seem easy going. (Participant 10)
The issues of capacity and problems with staff shortages have been highlighted by some researchers attempting to elucidate the impact of the staffing levels of nurses and the mix of nursing personnel in hospitals on patient satisfaction. For example, one study argues that hospital administrators, accrediting agencies, insurers, and regulators should take action to ensure that adequate nursing staff are available to protect patients and to improve the quality of care (Needleman and Buerhaus 2002). The current study found that good accessibility to health care – in terms of waiting times and availability of oncology ward staff (doctors, nurses) – are important factors influencing patient satisfaction in the KSA.
- Non-disclosure in the KSA setting
5.5 Summary of key qualitative findings
The qualitative phase of the current study has explored the ways in which interpersonal aspects of care and accessibility to health care influence patient satisfaction in an oncology ward setting at the SRCC in Riyadh. It has considered the role of cultural and organisational factors relevant to the health care context, as well as within the wider KSA society, in influencing these satisfaction levels. Four key themes have been identified and explored: (1) the doctor-patient relationship, (2) the nurse-patient relationship, (3) contextual factors relevant to cancer in the KSA, and (4) organisational factors.
A strong emphasis on the psychological as well as physical elements of care was evident; with many patients highlighting that doctor should understand and respond well to psychological state. Nurses’ interpersonal skills were deemed important and impacts on the quality of their experience. Largely, nurses were seen as supportive and understanding. However, some patients perceived the nurses as lacking in compassion and responsiveness, although this was also linked with nursing shortages and the observed lack of time that nurses had to interact with patients. In addition, it is attributable to the non-disclosure policies variability that instructs some nurses not to communicate certain health information to patients.
In relation to KSA contextual factors, it is evident that cultural perceptions of the doctor as a figure of authority and power in relation to one’s health often engendered a top-down power dynamic, where patients felt constrained about asking questions or interacting with doctors. However, other patients recognised the need for a more balanced dynamic of trust and rapport. In addition, there was evidence to suggest doctors are increasingly sharing information with patients themselves rather than with their families, as has historically been the norm in KSA. This departure from longstanding non-disclosure policies appears to promote patient satisfaction.
The multicultural care environment, comprising mainly expatriate nurses, had an impact on patient satisfaction levels. The language barrier with nurses who did not speak Arabic presented challenges to some patients and lowered their satisfaction with nursing care. In addition, the default English-speaking between doctors and nurses engendered a feeling of exclusion and anxiety among some patients.
The findings were mixed relating to patients’ perceptions of the SRCC’s operational efficiency and its impact on their satisfaction with care. While some participants praised the SRCC for its efficiency, environment and admission processes, many voiced strong views in their criticism of two main organisational factors: accessibility to health care and waiting times. These two factors were closely linked. Many patients noted having had to wait for long periods of time to be admitted to hospital, whether for a referral, or to gain access to a laboratory test or results. This, in turn, compromised their access to the treatment they needed and greatly lowered their levels of satisfaction with the services offered.
The norm of non-disclosure was considered a common factor that influenced patient satisfaction as seen through the analysis of the all the four themes and their subsequent subthemes. Non-disclosure is complex issue in KSA which contrasts to the general perception of non-disclosure in the Western context. In the Western context, the patient is the key individual who is responsible for the decision making in terms of treatment, interaction with doctors and nurses, and acquires crucial information about their health which they deem sensitive. This Western form of non-disclosure links very closely to doctor-patient confidentiality. However, in the KSA setting non-disclosure is the total opposite as analysed from the findings. Non-disclosure in the KSA setting means that information regarding the health of the patient is disclosed to the family of the patient, and the family decides which information is disseminated to the patient.
The current study’s qualitative findings add to the plethora of knowledge of interpersonal aspects that was focused on healthcare professionals exclusively. However, the current study expands to the knowledge of how interpersonal aspects of care coupled with service organisation influenced the level of patient satisfaction in the KSA oncology ward settings. Through the evidence extracted from the findings it can be concluded that patient satisfaction is closely linked to specific contextual factors that are related to the themes which have been discussed in this chapter.
[1] Sitters are commonly relatives of the patients who, at the patients’ request accompany them during their hospitalisation, offering moral and practical support. Typically, patients are required to ask for their doctor’s permission to have a sitter stay with them overnight.
Table 8 - Cross-tabulation of Gender, Age, Marital Status, Education, Home, and Patient Satisfaction
Table 8 - Cross-tabulation of Gender, Age, Marital Status, Education, Home, and Patient Satisfaction
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Age | older group | Count | 4 | 44 | 48 |
% within Age | 8.3% | 91.7% | 100.0% | ||
% within patients overall satisfaction | 30.8% | 50.6% | 48.0% | ||
% of Total | 4.0% | 44.0% | 48.0% | ||
younger group | Count | 9 | 43 | 52 | |
% within Age | 17.3% | 82.7% | 100.0% | ||
% within patients overall satisfaction | 69.2% | 49.4% | 52.0% | ||
% of Total | 9.0% | 43.0% | 52.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Age | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Gender | male | Count | 5 | 37 | 42 |
% within Gender | 11.9% | 88.1% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 42.5% | 42.0% | ||
% of Total | 5.0% | 37.0% | 42.0% | ||
female | Count | 8 | 50 | 58 | |
% within Gender | 13.8% | 86.2% | 100.0% | ||
% within patients overall satisfaction | 61.5% | 57.5% | 58.0% | ||
% of Total | 8.0% | 50.0% | 58.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Gender | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Marital status | single | Count | 5 | 16 | 21 |
% within Marital status | 23.8% | 76.2% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 18.4% | 21.0% | ||
% of Total | 5.0% | 16.0% | 21.0% | ||
married | Count | 7 | 58 | 65 | |
% within Marital status | 10.8% | 89.2% | 100.0% | ||
% within patients overall satisfaction | 53.8% | 66.7% | 65.0% | ||
% of Total | 7.0% | 58.0% | 65.0% | ||
divorced | Count | 0 | 4 | 4 | |
% within Marital status | 0.0% | 100.0% | 100.0% | ||
% within patients overall satisfaction | 0.0% | 4.6% | 4.0% | ||
% of Total | 0.0% | 4.0% | 4.0% | ||
widowed | Count | 1 | 9 | 10 | |
% within Marital status | 10.0% | 90.0% | 100.0% | ||
% within patients overall satisfaction | 7.7% | 10.3% | 10.0% | ||
% of Total | 1.0% | 9.0% | 10.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Marital status | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
Education | low education | Count | 5 | 35 | 40 |
%within Education | 12.5% | 87.5% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 40.2% | 40.0% | ||
% of Total | 5.0% | 35.0% | 40.0% | ||
high education | Count | 8 | 52 | 60 | |
%within Education | 13.3% | 86.7% | 100.0% | ||
% within patients overall satisfaction | 61.5% | 59.8% | 60.0% | ||
% of Total | 8.0% | 52.0% | 60.0% | ||
Total | Count | 13 | 87 | 100 | |
%within Education | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
patients overall satisfaction | Total | ||||
Less satisfied | Satisfied | ||||
5 | 39 | 5 | 39 | 44 | |
% within Respondents resident | 11.4% | 88.6% | 100.0% | ||
% within patients overall satisfaction | 38.5% | 44.8% | 44.0% | ||
% of Total | 5.0% | 39.0% | 44.0% | ||
Outside Riyadh | Count | 8 | 48 | 56 | |
% within Respondents resident | 14.3% | 85.7% | 100.0% | ||
% within patients overall satisfaction | 61.5% | 55.2% | 56.0% | ||
% of Total | 8.0% | 48.0% | 56.0% | ||
Total | Count | 13 | 87 | 100 | |
% within Respondents resident | 13.0% | 87.0% | 100.0% | ||
% within patients overall satisfaction | 100.0% | 100.0% | 100.0% | ||
% of Total | 13.0% | 87.0% | 100.0% | ||
4.2 Clinical Effectiveness of Doctors and Nurses
The following set of questions were used to capture doctors and nurses effectiveness. The questions under each of these headings were grouped into the following four categories:
Table 9 - Differential Measurement of the Effectiveness of Doctors and Nurses
Clinical Effectiveness of Doctors | Clinical Effectiveness of Nurses |
Technical Skills (Q1-3) | Technical Skills (Q12-14) |
Interpersonal Skills (Q4-6) | Interpersonal Skills (Q15-17) |
Information Provision (Q7-9) | Information Provision (Q18-20) |
Availability (Q10-11) | Availability (Q21-22) |
The respondents’ views on the clinical effectiveness of doctors and nurses are discussed in this section. Overall, these results indicate broad patient satisfaction with the technical and interpersonal skills, information provision, and availability of the doctors and nurses during their hospital stay in an Oncology ward in Riyadh.
4.2.1 Respondents’ View of Doctors Clinical Effectiveness
As shown in Table 10, respondents were most satisfied with the doctor’s medical follow-up (88%) and knowledge of illness (87%) in terms of their technical skills. Patient satisfaction ranged from 84 to 89% and 84 to 85% regarding the doctor’s interpersonal skills and information provision, respectively. Overall, respondents were least satisfied with the availability of doctors. Only 77% of them were pleased with the visitation time and 79% were happy with the frequency of doctor’s visits.
4.2.2 Respondents’ View of Nurses Clinical Effectiveness
Almost all of the respondents were satisfied with the nurse’s physical examination (94%). However, other technical skills (attention to comfort and care handling) only ranged from 81 to 84%, respectively. The majority of patients were satisfied with the nurse’s human quality (89%), but fewer patients were satisfied with their other interpersonal skills (74-78%). In terms of information provision, more respondents expressed satisfaction with the nurse’s information about treatment (82%). Overall, respondents were least satisfied with the availability of nurses representing 75% of satisfaction. Only 73% of respondents were happy with buzzer promptness (See Table 10).
Table 10 - Respondents’ View of Clinical Effectiveness and Service Organisation (n=100 patients)
Satisfied Satisfied | Less Satisfied Less Satisfied | |
Doctor’s Technical Skills Doctor's knowledge of illness | 87% | 13% |
Doctor's medical follow-up | 88% | 12% |
Doctor's attention to problems | 81% | 19% |
Doctor’s Interpersonal Skills Doctor's willingness to listen | 84% | 16% |
Doctor's interest in personality | 84% | 16% |
Doctor's support given | 89% | 11% |
Doctor’s Information Provision Doctor's information about illness | 85% | 15% |
Doctor's information about medical test | 84% | 16% |
Doctor's information about treatment | 84% | 16% |
Doctor’s Availability Doctor's frequency of visits | 79% | 21% |
Doctor's visitation time | 77% | 23% |
Nurse’s Technical Skills Nurse's physical examination | 94% | 6% |
Nurse's care handling | 84% | 16% |
Nurse's attention to comfort | 81% | 19% |
Nurse’s Interpersonal Skills Nurse's interest in personality | 74% | 26% |
Nurse's support given | 78% | 22% |
Nurse's human quality | 89% | 11% |
Nurse’s Information Provision Nurse's information about medical test | 74% | . 26% |
Nurse's information about care | 78% | 22% |
Nurses information about treatment | 82% | 18% |
Nurse’s Availability Nurse's buzzer promptness | 73% | 27% |
Nurse's devoted time | 75% | 25% |
Other Service and Care Organisation | ||
Discharge information provision | 86% | 14% |
Waiting time for medical test | 68% | 32% |
Speed of treatment | 68% | 32% |
Parking | 62% | 38% |
Department Access | 65% | 35% |
Hospital cleanliness | 85% | 15% |
4.3 Other Services and Care Organisation
Respondents were asked to rate other hospital services and care provided by the organization as a whole. The main categories of other services and care organization analysed are listed below.
Table 11 - Differential Measurement of Service and Care Organisation
4.3.1 Respondents’ View of Other Service and Care Organisation
As shown in Table 11 above, the respondents were more satisfied with discharge information provision (86%) and hospital cleanliness (85%). Respondents were less satisfied with the waiting time for medical test (68%), speed of treatment (68%), and department access (65%). Still, only 62% of them were satisfied with parking accessibility to the Oncology ward.
4.4 Factor Analysis of Observed Variables
An exploratory factor analysis was carried out in order to reduce the number of variables to useful factors and to identify the correlation among them. This section highlights the main results of factor analysis, which included descriptive statistics, reliability measurements, correlation matrix, total variance explained; communalities (i.e., proportion of variability of a variable that is explained by the factors); factor loadings (i.e., interpreted as Pearson correlation of an original variable with a factor); and extraction (i.e. variable reduction using principal component analysis)
4.4.1 Descriptive Statistics of Observed Variables
The above percentage results were also evident when calculating the mean of the observed variables. The highest mean indicates the less satisfaction level. In regard to doctors’ clinical effectiveness, respondents were more satisfied with their support (M=1.11, SD=.314) and least satisfied with their visitation time (M=1.23, SD=.423). In regard to nurses’ clinical effectiveness, respondents were more satisfied with their physical examination (M=1.06, SD=.239), but less satisfied with their buzzer promptness (M=1.27, SD=.446), and interest in personality (M=1.26, SD=.441). With respect to other services and organization, respondents were more satisfied with discharge information provision (M=1.14, SD=.349) and hospital cleanliness (M=1.15, SD=.359), but less satisfied with parking (M=1.38, SD=.488), department access (M=1.35, SD=.479), speed of treatment (M=1.32, SD=.469) and waiting time for medical test (M=1.32, SD=.469). (See Table 12).
Table 12 - Descriptive Statistics of Observed Variables
Mean(M) | Std. Deviation(SD) | Analysis N | |
Doctor's knowledge of illness | 1.1300 | .33800 | 100 |
Doctor's medical follow-up | 1.1200 | .32660 | 100 |
Doctor's attention to problems | 1.1900 | .39428 | 100 |
Doctor's willingness to listen | 1.1600 | .36845 | 100 |
Doctor's interest in personality | 1.1600 | .36845 | 100 |
Doctor's support given | 1.1100 | .31447 | 100 |
Doctor's information about illness | 1.1500 | .35887 | 100 |
Doctor's information about medical test | 1.1600 | .36845 | 100 |
Doctor's information about treatment | 1.1600 | .36845 | 100 |
Doctor's frequency of visits | 1.2100 | .40936 | 100 |
Doctor's visitation time | 1.2300 | .42295 | 100 |
Nurse's physical examination | 1.0600 | .23868 | 100 |
Nurse's care handling | 1.1600 | .36845 | 100 |
Nurse's attention to comfort | 1.1900 | .39428 | 100 |
Nurse's interest in personality | 1.2600 | .44084 | 100 |
Nurse's support given | 1.2200 | .41633 | 100 |
Nurse's human quality | 1.1100 | .31447 | 100 |
Nurse's information about medical test | 1.2600 | .44084 | 100 |
Nurse's information about care | 1.2200 | .41633 | 100 |
Nurses information about treatment | 1.1800 | .38612 | 100 |
Nurse's buzzer promptness | 1.2700 | .44620 | 100 |
Nurse's devoted time | 1.2500 | .43519 | 100 |
Information exchange | 1.1700 | .37753 | 100 |
Other staff helpfulness | 1.1600 | .36845 | 100 |
Admission information provision | 1.1900 | .39428 | 100 |
Discharge information provision | 1.1400 | .34874 | 100 |
Waiting time for medical test | 1.3200 | .46883 | 100 |
Speed of treatment | 1.3200 | .46883 | 100 |
Parking | 1.3800 | .48783 | 100 |
Department Access | 1.3500 | .47937 | 100 |
Hospital cleanliness | 1.1500 | .35887 | 100 |
Patients’ overall satisfaction | .8700 | .33800 | 100 |
4.4.2 Reliability Measurements
The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy index should be greater than 0.5 in order to support the use of a factor analysis and ensure that it is satisfactory. Large values for KMO commonly indicate that a factor analysis of the variables is considered a reasonable step to be taken. On the other hand, Bartlett’s sphericity test was used to test the null hypothesis that the population correlation matrix is uncorrelated (Mertler and Vannatta, 2010). Once the observed significance level is 0.0000 it is considered to be small enough to reject the hypothesis. The KMO coefficient was .820, which is close to one and the associated Sig. value of the Bartlett’s test was significant, p <.001; therefore, the null hypothesis is rejected. The results obtained confirm the sample size is adequate for conducting a factor analysis as the relationship between the variables is strong. The variables have some degree of correlation between them making it a rational idea to proceed with a factor analysis. See appendix 12 for KMO test Table1.
4.4.3 Correlation Matrix
A correlation matrix was utilized to further examine the strength, direction, and significance of the relationship between the variables. The strongest positive correlations were between nurse’s information about care and nurse’s information about medical test (r = .79, p <.001); and nurse’s information about treatment and nurse’s information about care (r =.69, p<.001), which were both statistically significant. The weakest positive correlations were between doctor’s information about illness and doctor’s medical follow-up (r =.02, p =.87); and nurse’s human quality and doctor’s information about medical test (r =.02, p =.83), which were not statistically significant. In contrast, the strongest negative correlations were between patients’ overall satisfaction and doctor’s support given (r = -5.29, p<.001) and patients’ overall satisfaction and nurse’s physical examination (r= -5.28, p<.001), which were statistically significant. The weakest negative correlations were between nurse’s human quality and doctor’s support given (r = -.02, p = .83) and patients’ overall satisfaction and speed of treatment (r = -1.81, p=.07), which were not statistically significant.
4.4.4 Total Variance Explained
The Total Variance Explained provided the eigenvalues of any contributing components and the percent of variance explained by the each component. A total of eight components were retained because they had eigenvalues which exceeded 1, as shown in appendix 13. After rotation, Component 1 accounted for only 12.39% of the total variance explained by the original variables, while Component 8 only accounted for 6.41%.
4.4.5 Communalities
Communalities show how much of the variance in the variables has been accounted for by the extracted factors. High communalities indicate a more reliable factor analysis. Communalities results shown in appendix 14 revealed nurse’s information about medical test explained 82.7% of variance, followed by other staff helpfulness (80.6%), nurse’s information about care (79.5%) and doctor’s information about illness (79.4%). Only three variables (doctor’s knowledge of illness, nurse’s buzzer promptness, and doctor’s willingness to listen) fell below the recommended .60.
4.4.6 Factor Loadings
Factor loadings (see appendix 15) illustrates how variables were loaded into components after rotation based on their coefficient size. An assessment of component loadings was necessary in order to label each component. The variable with the highest loading was hospital cleanliness (.825), followed by doctor’s information about illness (.818) and nurse’s information about care (.795).
4.4.7 Extraction
Principal component analysis was conducted utilizing a varimax rotation. The analysis retained the eight components. Table 13 provides the assigned names given to each component based on the highest factor loadings. The first component comprises items 12, 13,17,21,22 named Nurse Skills. Second component, includes items 18-20 named Nurse Information provision. Third component contains items 2, 4, 9 named Doctor Skills. The fourth component includes items 23, 24 named Staff helpfulness. The fifth component comprises items 27, 28 named Promptness of and accessibility to health care. The sixth component includes items 10 and 31 named doctor support and hospital environment. The seventh component contains items 7, 11 named doctor information provision and availability. The last eighth component comprises items 25, 26 named staff information provision.
Table 13 - Component Loadings and Eigenvalue by Varimax rotation
Factor name Items loaded in the factor | Factor Loading | Eigenvalue | % Variance | |||
Component 1 (FAC1_2): Nurse Skills | 3.96 | 12.39 | ||||
Nurse’s devoted time | .757 | |||||
21 Nurse’s buzzer promptness | .664 | |||||
12 Nurse’s physical examination | .648 | |||||
17 Nurse’s human quality | .641 | |||||
13 Nurse’s care handling | .641 | |||||
Component 2 (FAC2_2): Nurse Information Provision | 3.38 | 10.59 | ||||
Nurse’s info about care | .795 | |||||
Nurse’s info about medical test | .781 | |||||
Nurse’s info about treatment | .724 | |||||
Component 3 (FAC3_2): Doctor Skills | 3.02 | 9.46 | ||||
Doctor’s medical follow-up | .689 | |||||
Doctor’s willingness to listen | .598 | |||||
Doctor’s info about treatment | .580 | |||||
Component 4 (FAC4_2): Staff Helpfulness | 2.58 | 8.07 | ||||
Other staff helpfulness | .762 | |||||
Information exchange | .733 | |||||
Component 5 (FAC5_2): Promptness of and Accessibility to Healthcare | 2.53 | 7.91 | ||||
Speed of treatment | .773 | |||||
Waiting time for medical test | .662 | |||||
Parking | .629 | |||||
Component 6 (FAC6_2): Hospital Environment and Doctor Support | 2.50 | 7.84 | ||||
Hospital cleanliness | .825 | |||||
Doctor’s frequency of visits | .652 | |||||
Component 7 (FAC7_2): Doctor Information Provision and Availability | 2.43 | 7.60 | ||||
Doctor’s info about illness | .818 | |||||
Doctor’s visitation time | .587 | |||||
Component 8 (FAC8_2): Staff Information Provision | 2.05 | 6.41 | ||||
Discharge info provision | .739 | |||||
Admission info provision | .711 |
4.5 Binary Logistic Regression
Using the resulting factor scores from the factor analysis and the socio-demographic variables, four binary logistic regressions were performed to evaluate the degree of association in these determinants on patients’ overall satisfaction. The findings are presented in the subsequent sections.
4.5.1 Doctor’s Clinical Effectiveness and Patients’ Overall Satisfaction
For this analysis, the independent variables were Doctor Skills (FAC3_2), and Doctor Information Provision (FAC7_2) and dependent variable was overall satisfaction. Model fit statistic shown in appendix 16 Table 1 indicates a fairly good-fitting model -2 Log Likelihood = 58.427. The two components, Doctor Skills and Doctor Information Provision and Availability, accounted for nearly 32% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 11.309 and its associated Sig. value was not statistically significant, p = .13. Appendix 16 Table 2 presented the classification results, which indicated the model correctly classified 89.0% of cases.
The summary of model variables displayed in Table 14 revealed the odds ratios; however, the Wald statistics for one component (Doctor technical and interpersonal Skills) was not significant, p = .16. Therefore, the null hypothesis was retained for this component.
Table 14 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | Doctor technical & interpersonal skills FAC3_2 | -.417 | .295 | 1.995 | 1 | .158 | .659 | .370 | 1.175 |
Doctor information provision FAC7_2 | -1.163 | .306 | 14.489 | 1 | .000 | .312 | .172 | .569 | |
Constant | 2.417 | .414 | 34.092 | 1 | .000 | 11.208 | |||
a. Variable(s) entered on step 1: FAC3_2, FAC7_2. | |||||||||
The logistic regression coefficients give the change in log odds of the outcome based on a one unit increase in the variable. For every one unit change in Doctor Information Provision and Availability, the log odds of overall satisfaction increases by 0.312, as seen in Table 14 above. This was the only component that significantly contributed to the model, p<.001.
4.5.2 Nurse’s Clinical Effectiveness and Patients’ Overall Satisfaction
For this analysis, the independent variables were Nurse Interpersonal and Technical Skills (FAC1_2) and Nurse Information Provision (FAC2_2), and the dependent variable was overall satisfaction. Model fit statistic shown in appendix 17 Table1 indicates a fairly good-fitting model -2 Log Likelihood = 54.396. The two components, Nurse Interpersonal and Technical Skills, and Nurse Information Provision, accounted for 38% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 6.940 and its associated Sig. value was not statistically significant, p = .44. As shown in appendix 17 Table2, the results of the classification table revealed the model correctly classified 90% of cases.
The summary of model variables displayed in Table 15 revealed the odds ratios; however, the Wald statistics for one component (Nurse Information Provision) was not significant, p = .54. Therefore, the null hypothesis was retained.
Table 15 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | Nurse interpersonal & Technical Skills FAC1_2 | -1.283 | .319 | 16.165 | 1 | .000 | .277 | .148 | .518 |
Nurse information Provision FAC2_2 | -.201 | .328 | .375 | 1 | .540 | .818 | .430 | 1.555 | |
Constant | 2.455 | .423 | 33.747 | 1 | .000 | 11.646 | |||
a. Variable(s) entered on step 1: FAC1_2, FAC2_2. | |||||||||
The logistic regression coefficients give the change in the log odds of the outcome based on a one unit increase in the variable. For every one unit change in Nurse Interpersonal and Technical Skills, the log odds of overall satisfaction increases by 0.277, as seen in Table 15 above. This was the only component that significantly contributed to the model, p<.001.
4.5.3 Service and Care Organisation and Patients’ Overall Satisfaction
For this analysis, the independent variables were Promptness of and Accessibility to Healthcare (FAC5_2), Staff Information Provision (FAC6_2), Staff Helpfulness (FAC4_2), and Hospital Environment and Doctor Support (FAC8_2), and the dependent variable was overall satisfaction. Model fit statistics shown in appendix 18 Table 1 indicates a fairly good-fit, -2 Log Likelihood = 68.020. The four components, Promptness of and Accessibility to Healthcare, Staff Helpfulness, Hospital Environment and Doctor Support, and Staff Information Provision, accounted for about 16% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 6.307 and its associated Sig. value was not statistically significant, p = .61. As shown in appendix 18 Table 2, the model correctly classified 87% of cases.
The summary of model variables displayed in Table 16 provided the odds ratios; however, the Wald statistics for three components (Staff Helpfulness, Promptness of and Accessibility to Healthcare, and Staff Information Provision) were not significant (p>.05). Therefore, the null hypothesis was retained for these components.
Table 16 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | Staff Helpfulness FAC4_2 | -.163 | .263 | .381 | 1 | .537 | .850 | .507 | 1.424 |
Promptness &accessibility to Healthcare FAC5_2 | -.361 | .307 | 1.379 | 1 | .240 | .697 | .382 | 1.273 | |
Hospital environment & doctor support FAC6_2 | -.555 | .252 | 4.845 | 1 | .028 | .574 | .350 | .941 | |
Staff Information Provision FAC8_2 | -.428 | .271 | 2.499 | 1 | .114 | .652 | .383 | 1.108 | |
Constant | 2.142 | .352 | 37.031 | 1 | .000 | 8.517 | |||
a. Variable(s) entered on step 1: FAC4_2, FAC5_2, FAC6_2, FAC8_2. | |||||||||
The logistic regression coefficients give the change in the log odds of the outcome based on a one unit increase in the variable. For every one unit change in Hospital Environment and Doctor Support, the log odds of overall satisfaction increases by 0.574 as seen in Table 16 above. This was the only component that significantly contributed to the model, p=.03.
4.5.4 Socio-demographic Characteristics and Patients’ Overall Satisfaction
For this analysis, the independent variables were gender, age, marital status, residence, and education, and the dependent variable was overall satisfaction. Model fit statistic shown in appendix 19 Table1 indicates a poor fitting model, -2 Log Likelihood = 72.798. The five socio-demographic variables accounted for approximately 8% of the explained variance in patients’ overall satisfaction.
The final model did not significantly differ from the empty model (i.e., model without variables). The Chi-square value was 5.762 and its associated p value was not statistically significant, p = .67. Appendix 19 Table 2 presented the classification results, which indicated the model correctly classified 87.0% of cases.
The summary of model variables displayed in Table 17 revealed the odds ratios; however, the Wald statistics for the socio-demographic variables (gender, age, marital status, education and residency) were not significant (p>.05). Therefore, the null hypothesis was retained.
Table 17 - Regression Coefficients
Regression Coefficients | |||||||||
B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I.for EXP(B) | |||
Lower | Upper | ||||||||
Step 1a | AGE(1) | .595 | .781 | .580 | 1 | .446 | 1.813 | .392 | 8.375 |
Gender(1) | .376 | .680 | .306 | 1 | .580 | 1.457 | .384 | 5.520 | |
M.STATUS | 1.177 | 3 | .759 | ||||||
M.STATUS(1) | -.691 | 1.471 | .221 | 1 | .638 | .501 | .028 | 8.944 | |
M.STATUS(2) | .104 | 1.257 | .007 | 1 | .934 | 1.110 | .094 | 13.039 | |
M.STATUS(3) | 19.397 | 20016.756 | .000 | 1 | .999 | 265484571.007 | .000 | . | |
EDUCATION(1) | .118 | .629 | .035 | 1 | .851 | 1.126 | .328 | 3.865 | |
RESIDENCE(1) | .041 | .640 | .004 | 1 | .949 | 1.042 | .297 | 3.655 | |
Constant | 1.524 | 1.371 | 1.236 | 1 | .266 | 4.590 | |||
a. Variable(s) entered on step 1: AGE, Gender, M.STATUS, EDUCATION, RESIDENCE. | |||||||||
4.6 Summary and Interpretation of the Results
The quality of the data was important in assuring the reliability and validity of the results. The quality of the data was established by selecting a representative sample of participants. The data was collected from participants who were all patients in oncology wards. The data collected was through the adapted EORTC 32 INPATSAT validated, Arabic pilot test and questionnaire. The sample size was evaluated using a KMO test and found to be of an adequate size. The data analysis was carried out in such a way that no data was lost or distorted
Generally, most respondents’ satisfaction level with the services received was very high (87%). These results support previous findings mentioned in the literature review that high scores are usually reported in patient satisfaction surveys. The study showed that females (50%), married (58%), highly educated (60%), and resided outside of Riyadh (56%) were more satisfied with the services received during their stay in the Oncology wards.
The exploratory factor analysis was conducted to determine what, if any, underlying structures existed for 32-items of the EORTC IN-PAT32 questionnaire, and to describe and summarize the relationship between this given set of variables. Principal component analysis identified eight factors and they are as follows: Nurse Interpersonal and Technical Skills (5 items), Nurse Information Provision (3 items), Doctor Skills (3 items), Staff Helpfulness (2 items ), Promptness of and Accessibility to Healthcare (3 items) , Hospital Environment and Doctor Support (2 items) , Doctor Information Provision and Availability (2 items), and Staff Information Provision (2 items). These components enabled relationships between responses of patients with regard to their satisfaction to be analysed and allowed for the measurement of the patient’s level of satisfaction. The identified components may assist future research on patient satisfaction in a KSA oncology ward settings.
Binary logistic regression analyses were performed to determine which component loadings and socio-demographic characteristics were significant contributors to patients’ satisfaction. Regression analysis indicated that the factors that were important for overall patient satisfaction were: 1) Doctor Information Provision and Availability, 2) Nurse’s Interpersonal and Technical Skills, 3) Hospital Environment and Doctor Support However, none of the socio-demographic variables were important for overall patient satisfaction
Further exploration into why patients seemed generally satisfied with the care and services provided was necessary. In order to gain deeper insight and understanding, semi-structured interview questions were developed based on the resulting component loadings from the factor analysis. The integration at this intersection of phase 1 quantitative analysis and phase 2 qualitative semi structured interviews was designed to collect high quality data on patient satisfaction.
A discussion of the findings presented here, along with those from Phase 2 (chapter 5), is then provided in chapter 6, where the complementarity of the quantitative and qualitative data is shown. The process of integrating the findings on patient satisfaction in oncology ward settings which was collected from both phases is thoroughly detailed in chapter 6. The implications of the findings and considerations for practice and future research are also considered in chapter 6.
Chapter 5 - Qualitative Findings
5.1 Introduction
In this chapter, the findings from Phase 2 are presented. The organisation of this chapter compiled in order to produce information that will help in answering the research question of the current study; what factors contribute to or hinders patient satisfaction with care in oncology wards in the SRCC? The chapter is organised thematically based on themes that emerged during the interviewing process of the participants. The chapter begins with a summary of socio-demographic characteristics of the respondents which provides insights into the demographic trends of the respondents from which data on patient satisfaction is drawn. The remaining sections of the chapter (5.3.1-5.3.4) categorise the findings of the interview data using themes based on the results obtained from the interviews. These themes are considered as factors which impact patient satisfaction.
Each of the subsections under section 5.3 provide an in-depth understanding of interpersonal aspects of care and accessibility of health care as influential factors that formulate adult oncology patients’ perception of their satisfaction. The findings within these subsections aided in fulfilling the aims of the current study.
To further achieve the aims of the current study, each key theme is presented separately, with relevant examples from the translated interview extracts. These interview extracts were selected based on the coding process and also to represent the wide range of participants’ views. Commentary is provided to link these findings with the literature, where appropriate, and also to highlight any similarities and differences between participants’ responses. The chapter concludes with a summary of the key findings from this second phase of the study.
5.2 Socio-demographic patient characteristics
In Table 1, the socio-demographic details of the participants, outlining their age, gender, education level, marital status and place of residence are presented. It should be noted that there were a high number of young people participating in the study. This high proportion of younger people (<45 years) was due to the largely self-selecting aspect of this part of the research, since the choice of interviews was based on those who volunteered. This may have made the sample unrepresentative of the general target population, since the average median age of the diagnosis of cancer for a man was 58 years of age and 51 for women, in 2010 ( Saudi Cancer Registry 2010). While the current study portrays an age for a man as 46-55 years old or 66-75 years old and for women a median age of 36-45 years olds. The current study’s sample is not reflective of cancer incidence/prevalence in KSA but is a mere reflection of the participants that had volunteered to take part in the study.
Table 1 - Patient socio-demographic characteristics
Age | Gender | Education | Marital status | Residency |
36-45Y | Female | High school | Married | Riyadh |
46-55Y | Female | Primary | Married | Riyadh |
36-45Y | Female | High school | Married | Riyadh |
26-35Y | Female | University | Married | Outside Riyadh |
36-45Y | Female | High School | Divorced | Riyadh |
36-45Y | Male | Intermediate | Married | Outside Riyadh |
18-25Y | Female | Intermediate | Single | Outside Riyadh |
26-35Y | Female | High School | Married | Outside Riyadh |
36-45Y | Female | Illiterate | Married | Outside Riyadh |
36-45Y | Female | High School | Married | Outside Riyadh |
66-75Y | Male | Primary | Married | Riyadh |
46-55Y | Female | Primary | Widowed | Riyadh |
46-55Y | Female | University | Married | Riyadh |
56-65Y | Female | Intermediate | Widowed | Riyadh |
46-55Y | Male | Intermediate | Married | Riyadh |
46-55Y | Female | Intermediate | Married | Outside Riyadh |
46-55Y | Female | University | Married | Outside Riyadh |
36-45Y | Female | University | Married | Outside Riyadh |
26-35Y | Female | High school | Single | Outside Riyadh |
Above 76Y | Female | Primary | Married | Outside Riyadh |
18-25Y | Female | High school | Single | Outside Riyadh |
36-45Y | Female | University | Married | Outside Riyadh |
Based on Table 1, of the 22 participants only two were male. Both of whom were married and resided in Riyadh. However, of the two male participants, one aged between 66- 75 years had only attained primary education while the other male participant aged 45- 55 years old attained intermediate education. The remaining 20 participants were females of varied age, marital status, and education level. The median age of females within the sample was 36-45 years old. Of the female participants 13 were married, 3 were single, 2 were widowed and one was divorced. A majority of the female participants resided outside of Riyadh (11) while the remaining (7) resided in Riyadh. All the female participants except one had attained some level of education. A majority of the participants (7) had attained a high school level education, while the remaining were dispersed with 3, primary, 3 intermediate, and 5 university level education amongst the participating females.
5.3 Key themes emerging from the interview data
The four primary themes identified from interview data are shown in Table 2 and are discussed in extent in the sub-sections.
Table 2 - Themes and Subthemes that Emerged from the Interview Data
Themes | Subthemes |
The doctor-patient relationship | Perception of doctor- patient relationship |
Interpersonal communication | |
The nurse-patient relationship | General perception of nurse-patient relationship |
Technical aspects of nurses’ skills | |
Interpersonal aspects of nurses’ skills | |
KSA cancer contextual factors | Perception of cancer |
Power dynamic of KSA Doctor | |
Religious influence | |
Family influence | |
Multi-cultural environment–nurses’ affects | |
Organisational factors : service organisation | Perception of general service organisation |
Accessibility | |
Waiting times for services |
5.3.1 The doctor-patient relationship
The analysis of participants’ descriptions of their interactions with their doctors provides insights into the aspects of the doctor-patient relationship that are especially meaningful to the patient and influence their understanding of their experiences and the satisfaction with the care they receive.
The doctor-patient relationship in KSA is somewhat different to the western model. The family often needs to be consulted concerning the doctor’s disclosure of information to a patient. Doctors are often required to inform a patient’s family of their treatment and health. This means that the doctor-patient relationship is more complex and that a doctor needs to consider the family in their relationship with their patient. Many patients in the KSA are comfortable with this, because of cultural considerations. However, this particular take on non-disclosure has a significant impact on patient satisfaction and restrains the KSA healthcare delivery from becoming patient-centred. This in turn may have a significant impact on the findings of the study. It is possible that since females are not participant in the delivery of their healthcare they will be less satisfied than compared to male patients. However, although male patients are involved in their healthcare and treatment options, they may not be as satisfied as ultimately the decision for treatment and discussion of patient health status is discussed by the patient’s family. The issue of non-disclosure causes patient dissatisfaction due to their experience with having their health information disclosed to people other than themselves and treatment decisions making be left to individuals other than themselves.
Four main factors were identified that represent aspects of interpersonal communication between doctors and their patients:
- Listening: listening to and addressing the patients’ questions and concerns
- Information provision: providing adequate information about the patients’ conditions and treatments
- Motivation: being encouraging and motivating to the patients
- Care and compassion: being caring and compassionate, with attention to the patients’ psychological as well as medical needs.
These aspects are important to the relationship between patient and doctor despite the requirements for non-disclosure. Based on the analysis of the findings, doctors functioning within the KSA healthcare delivery environment are unable to appropriately deliver these interpersonal communications due to the distraught non-disclosure policy that is family centred. There have been attempts by doctors to do so as evident from the analysis of the findings. Non-disclosure in the KSA setting is influenced by cultural norms, religious beliefs, and attitudes of the doctors. For example, female patients need to have a male guardian who makes the ultimate decisions regarding their healthcare, this will include deciding between treatment options. Therefore, patient information is disclosed to the male guardian of the patient which is ultimately against the philosophical and legal context of non-disclosure. However, this necessary for the doctor to do as it conforms to cultural beliefs of KSA.
The following section presents the participants’ general perceptions of the doctor- patient relationship in the oncology ward at the SRCC in Riyadh. In the subsequent sections the four sub-themes are examined in detail.
5.3.1.1 General perceptions of the doctor-patient relationship
The current study produced varied views among participants regarding the doctor-patient relationship experience. Many built their relationship with their patient in a way that was satisfying, although they were dissatisfied with some aspects.
Fourteen of the twenty-two research participants in the study were positive about their experiences of the doctor-patient relationship. They expressed appreciation and gratitude for their doctors’ personal qualities and interpersonal skills, which had clearly contributed to satisfaction with their hospital stay, despite the non-disclosure requirements that were implemented on all patients including the current study’s sample of 22. Those reporting positive experiences described their doctors in terms such as comforting, trustworthy, helpful, kind, co-operative and patient. For example, two participants stated the following:-
They are so patient and obliging, and dealing with them is easy and comfort(able). (Participant 2)
However, eight participants were critical of some aspect of the doctor-patient relationship. They commented that, although the doctors’ medical expertise was of a very high standard, they were lacking in interpersonal skills, including communication skills, kindness, empathy, and compassion. These views may have been in part influenced by the non-disclosure requirements of their families. Families were consulted by the doctor in regards to the patient treatment options and updates. The eight respondents were not involved in the decision making of their treatment. Crucial care options and information was not disclosed appropriately to patients but was left to the families. This lack of non-disclosure causes patients to feel that doctors are not communicating with them properly when it comes to disclosing information that aids the patient in decision making in regards to their health. The following extracts from participants’ narratives illustrate this:
They told me about chemotherapy and sent me to the health educator to explain the cycles and side effects, which was good. But the doctors here didn’t give the whole treatment plan or future plan to clarify things for me more. (Participant 3)
Because many families restrict information disclosure this prohibits doctors from disclosing information to some patients, especially females. Doctors often need to consult patients’ families on providing information or what should be revealed. This can lead many patients to not being fully informed of their treatment. In fact, many patients are not aware of this family request and the restrictions that it places upon doctors’ level of communication with their patient, especially with regard to the disclosure of treatment plans. This may cause some patients, especially females, to believe that their doctors are poor communicators, while in fact they are only conforming to the families’ wishes.
Indeed, there was no indication that doctors were avoiding contact with these patients. However, in some cases the doctors’ communications with their patients were not satisfying experiences. Females and males are treated differently under the non-disclosure arrangements. However, several males, expressed their opinion that doctors have ‘poor communication’ and this suggests that some patients perceive their communications with doctors as being unsatisfactory.
5.3.1.2 Listening skills
Participants reported that they often had questions and concerns about their illness or treatment, which, if not answered, caused great anxiety and stress. It was important to them to have adequate opportunities to ask their doctor questions or discuss their concerns, and to feel comfortable in doing so. The fourteen participants who mostly expressed satisfaction with the doctor-patient relationship all indicated that their doctors were frequently available to them, encouraged them to ask questions, and provided all the information needed to address their concerns, as the following extracts demonstrate:
They made me comfortable enough to share my concerns with them and patiently listened to me. They answered each of my queries and cleared my doubts. (Participant 15)
They have been very kind and patient. They listen to my concerns and give complete attention to what I say … They answer all my questions no matter how foolish my questions might sound. (Participant 9)
These data show that the majority of the participants were experiencing high levels of personal attention from their doctors, providing evidence of optimum listening skills in the hospital, and indicating that the doctors are addressing the concerns and psychological needs of their patients. This was the case with both males and females and suggested that doctors displayed good communication skills despite the limitations imposed upon them by the non-disclosing cultural attitude. Communication involves issues like ‘listening’ which would not be greatly influenced by any non-disclosure requirements.
In contrast, eight participants reported negative experiences of communicating with their doctors, which they perceived as mainly owing to the doctors’ busy routines and limited time for patient conversations. These participants commented that the doctors seemed unwilling to listen to their questions and concerns, or to provide the information being sought. The following extracts demonstrate this, and also highlight the power dynamics implicit in these doctor-patient relationships:
I … didn’t have the courage to stop them or ask them more as they look busy and just talk quickly during rounds. (Participant 5)
This participant’s concerns and emphasis on his/her own lack of courage convey a state of being afraid to engage doctors in conversation, which may or may not be related to the doctors’ actual listening capacity. However, the subsequent observations made by other participants indicate that this listening capacity may be limited, in some cases:
My talk with them is usually very brief and one sided in which all I had to say was ‘yes’ or ‘no’; they tell and I listen. (Participant 6)
The doctors asked me general questions but were never interested in my specific concerns. (Participant 21)
These comments suggest a power dynamic that is downwards directed from doctor to patient, where the doctor is the one in control of the knowledge that the patients need in order to allay their anxiety. The fact that this anxiety is not adequately listened to, and the knowledge is not shared, highlights an unequal balance of power and control in the patient-doctor relationship here. In particular, the repeated reference to ‘fear’ and ‘courage’ demonstrate the distress some participants felt at not being adequately listened to.
These findings indicate that at least some of the oncology doctors treating the participants in the current study did not give the impression that the participants’ concerns are not of interest. Previous research by Jagosh et al. (2011) argues that physician listening has three very important functions: (1) clinical data gathering, (2) healing and therapeutic value, and (3) building the doctor-patient relationship. While it is uncertain from my findings whether or not the doctors were actually listening to the concerns of their patients, what the study does show is that some felt that they were not being heard. As Ansmann et al. (2013) found, a busy hospital work environment and heavy workload may hinder physicians’ ability to adequately support patients and they may feel constrained in communicating with patients because of any non-disclosure arrangements.
5.3.1.3 Information provision
Most participants reported positive experiences of receiving comprehensive information from their doctors, and noted the calming and reassuring effects that these had on them. The following extracts illustrate this:
The doctors listened to my queries and clarified my doubts in detail. They took every step to inform me well at the start of treatment and also provided me with relevant information during the course of treatment. (Participant 16)
I even had some misconceptions about radiology but they clarified the concepts and now I’m not scared of my treatment. (Participant 11)
These statements would indicate that despite any non-disclosure arrangements in many cases doctors are, in fact, listening to patients and offering them information on their treatment. They are able to clarify a patient’s treatments in a general way and in doing so keep patients somewhat informed. These participants’ statements provide a contrast to some of the more negative perceptions of doctors’ listening skills described in the previous section. Of note is the frequent referral of participants to their lack of clarity regarding their illness and treatments. The responses here, however, certainly suggest some doctors’ efforts to alleviate patients’ anxiety regarding the course of their disease and treatment (even if the prognosis itself may not be positive) through adequate information provision.
It did appear that information provision was problematic for some participants; some reported having to wait too long to receive the information they needed. This was at least partly due to the doctors’ busy schedules, and partly due to the hospital protocol arising from policies of the KSA health service, which prevents the nursing staff from providing certain information to patients. As one participant said:
I am waiting longer to get information about results from doctors, while nurses can’t give me this information until the doctors do their round. I sometimes can’t tolerate the nurses saying that they are unsure about my treatment, as they have to wait for the results and for the doctor to read the results and inform me about progress. This process makes me feel more worried and anxious about my stay. (Participant 5)
Even though some data showed a positive trend toward taking patient satisfaction into account, participant responses such as these indicate that organisational factors such as hospital policies or procedures can sometimes adversely affect the experience of patients and have a negative impact on patient well-being (Aljubran, 2010). The following comments highlight this:
It’s worrisome and irritating to wait so long. Especially for cancer patients, it’s even more irritating to wait. I don’t like it when hospital management forget about the psychological state of their patients. (Participant 13)
I had even requested my oncology team twice to come quickly for the referral visit. They didn’t pay any attention and I’m still here waiting for my psychologist session. I feel so dissatisfied and depressed. (Participant 10)
The stark contrast between these perceptions and those of the participants who were satisfied with the quality and timing of the information they had received conveys high variability in the level of information provision among different doctors at the hospital. What is apparent from these extracts is that long waiting times to receive information can substantially increase patients’ stress levels. Addressing this issue is important since studies have shown that psychological distress has an impact on cancer mortality (Hamer et al, 2008). For example those individuals who expressed dissatisfaction with the doctors’ communication skills could be at risk of poorer health outcomes. This would support the view that non-disclosure could be interfering with a patient’s health.
5.3.1.4 Motivation
The data from the interviews support the evidence that the nature, as well as the level of communication between doctor and patient has a significant influence on patient satisfaction and how it is perceived (Mobiereek et al. 1996; Ezubair 2002). It is clear from participants’ statements that doctors potentially play an essential role in raising and maintaining patient morale, by being encouraging and positive about their recovery:
They advise me to keep myself hopeful. They tell me that I can get healthy again and I’ll be able to live a normal life. I’m so determined to get rid of my breast cancer and I’m thankful to my doctors that they have been helping me so much. (Participant 9)
They were supportive in the success of the treatment. They were encouraging and kind. They sounded like they truly wanted me to get well. (Participant 3)
The key elements here are the nurturing of hope, encouragement, and the perception of genuine well-wishing on the doctors’ part. The doctors’ positive attitudes and the nature of patients’ communication with them may reflect, at least in part, the culture of the KSA, in which physicians are traditionally held in high regard and as figures of authority (Mobeireek et al.1996; Younge et al. 1997; Aljubran 2010). However, in contrast to the negative dynamic of power and control, the findings suggest that there were few doctors who were perceived as listening inadequately to their patients’ needs were not viewed favourably by patients. The doctor’s ability to listen is described as deeply appreciated and seen as responsibly used, i.e. for the psychological improvement of the patient. Being in the position of authority means that compared to other members of the health care team, doctors have a greater impact, either positive or negative, on the health and wellbeing of patients. There were mixed views that appeared in the investigated which included that some of the participants expressed being motivated and encouraged by their doctors which is evident from the quotes below, attesting that communication and relationship with doctors is a significant factor in enhancing patients’ psychological well-being;
I myself didn’t want to stay as I felt depressed, but their motivating words helped me and I started being hopeful. Now, I can proudly say that if my doctors hadn’t stayed positive and supportive, I wouldn’t have been able to come out of my illness ever. (Participant 19)
They have inspired me with their attitude and kindness. They are encouraging, it becomes easier to hope for successful treatment … Their supportive words became my strength and here I’m ready to go home with a healthy body and healthy mind. (Participant 13)
However, the current study had also found contrasting views to those above, these especially surfaced when patients were questioned specifically about their relationships with their doctors.
When doctors are encouraging and motivating, this can be perceived as having a positive impact on the progression of the patient’s recovery. As previous research has indicated, doctors’ communication in an oncology setting can affect the level of patient satisfaction and may also influence the patient’s wellbeing and quality of life (Ong et al., 2000; Wildes et al., 2011).
The practice of non-disclosure could, especially for females, lead to them to build their experiences in a negative way and this in turn could impact upon their health outcomes. The implication of the non-disclosure as a cultural attitude could therefore mean that females are more likely to suffer a negative health outcome than males in KSA oncology settings.
Some participants reported that communication with their doctors had been negative, in the sense that their experiences with doctors were not constructed as encouraging or motivating. This is demonstrated by two participants, who explicitly stated how this had disheartened them and weakened their resolve to recover from their illness:
As medical attendants their behaviour has never been motivating or heartening. (Participant 10)
They have a very casual attitude which I don’t appreciate much. They don’t fill the patient with motivation and determination to fight against their illness. (Participant 6)
These positive and negative examples show the impact that the physician’s manner may have on the psychological state and even on the physical well-being of the patient. These examples also reflect on the connection between a healthy body and a positive mind, as ‘hope’ was a key word emerging in positive descriptions of doctors who were seen as motivating. Previous research argues that a patient’s attitude may be positively correlated with doctor behaviours that are perceived as encouraging and motivating, often resulting in positive medical outcomes such as improved adherence to treatment and self-care (Street et al. 2009). By being motivating and encouraging to the patient, doctors’ communication may have a significant impact on the patient’s state of mind, such as lowering anxiety, and thus, may indirectly influence the overall outcome of the illness episode (Ommen et al. 2010). While it has been argued that an awareness of psychological distress is an essential aspect of patient care, oncology doctors are often unwilling to note the distress in patients, and ask questions regarding patients’ psychological health (Cull et al. 1995; Fallowfield et al. 2001).
The interviews provide insights into the overall impact of a trusting and motivational relationship between the doctor and patient on patient satisfaction and well-being, and particularly on the patients’ abilities to cope with and fight their illness. Participants’ comments tend to support the findings of previous studies that have highlighted the association between a trusting doctor-patient relationship and patients coping with their illness, which may result in improved patient outcomes (Epstein and Street 2007; Arora 2008).
In the beginning of all this I was scared to death and every step of my treatment used to frighten me ... But when I talked about this with my doctors, they listened and gave such kind advice and motivation that finally I started to feel calm. (Participant 4)
The doctors were very friendly and took time to build up my confidence. This provided me with the strength to fight (the) suffering caused by the disease and treatment. I felt comfortable in their presence and that brought a lot of positive energy to me to receive the treatment with great hope and confidence. (Participant 16)
The interview data show a strong link between hope and trust, reiterating the notion of a positive power dynamic between doctors and patients, where the doctors are respected figures of authority who are seen as crucial to reassuring and encouraging the patient with whom they have built up a good relationship. Other research similarly indicates that having a trusting relationship with one’s doctor can have a positive impact on the patient’s mind, generating a more hopeful attitude towards the condition and thus aiding the overall mental state and self-care, which ultimately improves the patient’s quality of life (Clever et al. 2008). Trust could become an issue as a result of the non-disclosure by doctors of issues related to the patient’s treatment. However, there are multiple factors involved in patients’ construction of satisfaction, such as listening and if a doctor concentrates on these then any arrangements between the family and doctor about non-disclosure would not impact too negatively upon patients trust.
Exploring further the connection of trust with patients feeling motivated and encouraged by their doctors, it was found that where there was insufficient trust in the doctor’s genuine interest in the patient’s well-being, feelings of hope and encouragement suffered to the detriment of the patient’s emotional state. For example:
Doctors’ change in behaviour or attitude can make the patient feel ‘unwanted’. Depression and hopelessness take over his mind and his hopes to get healthy fade away. Fear, frustration and sadness fill his mind. (Participant 3)
These findings support evidence from other studies regarding the lack of a trusting doctor-patient relationship, which can negatively influence patients’ levels of satisfaction (Stewart 1995; Parker et al. 2003). It is evident from my findings that, if doctors fail to communicate in appropriate ways with patients, the lack of trust and subsequent lack of motivating and encouraging behaviour may adversely impact on the psychological wellbeing of the patient, and potentially on the clinical outcome.
My findings are similar to those of Fogarty et al. (1999) and Ommen et al. (2010), but additionally provide a deeper, more meaningful contribution to the hitherto poorly researched field of patient satisfaction from the perspective of the KSA context. It would also indicate that more disclosure of health information is important to enhance the doctor-patient relationship and this in turn – based on the evidence that good communications improve patients’ well-being (Aljubran, 2010) – would lead to better health outcomes for those being treated in an oncology setting.
5.3.1.5 Care and compassion
The analysis revealed that a further communication aspect that can have a significant influence on patient satisfaction is when doctors show compassion and care. The compassionate behaviour of physicians is defined by Carmel and Glick as ‘strong devotion to the welfare of the patient on two crucial dimensions of patient care: technical and socio-emotional’ (1996, p. 1253). Doctors perceived as caring and compassionate with patients may provide an element of emotional healing, which could be viewed as a determinant of patient satisfaction (Fogarty et al. 1999; Bertakis et al. 1999).
Many of the participants frequently reported experiences associated with compassion and caring exhibited by their doctors, using terms such as tender, understanding, patient, concerned, and reassuring, and indicating a broader definition of care and compassion. For example:
Doctors have been so tender and (re)assuring. (Participant 13)
The doctors were concerned about me and wanted me recover soon. (Participant 15)
Many also directly alluded to the concepts of compassion, or lack of compassion, when discussing the care they had received from doctors. The absence or presence of compassion clearly had an impact on patients’ overall level of satisfaction with their care. These findings evoke the understanding that an important dimension of patient satisfaction is the ability of the doctor to relate to and engage with the patient as an individual or, as highlighted in the 2001 IOM definition of the patient centred approach, to be concerned with the ‘needs, and values [of the patient], and ensure that patient values guide all clinical decisions’ (IOM 2001, p. 40).
The perceived lack of compassion may have been attributable to doctors’ avoiding close engagement with some patients due to the practice of disclosure of certain health information to families rather than patients. Another possible explanation is that expatriate doctors for whom Arabic is a second language experience difficulty verbally expressing care and compassion to Saudi patients. These expatriate doctors may feel in particular constrained about communicating with patients in the context of the requirements regarding the non-disclosure of information to patients.
The findings indicated that some participants had experienced compassion and care from their doctors according to these terms, which in turn helped them to feel more comfortable in discussing their concerns with the doctor; this also made them feel the doctor was truly interested in their recovery. The following extracts illustrate this:
The doctors were understanding about my need for a sitter[1] and sent me a social worker to facilitate that during my stay. (Participant 20)
The doctors were compassionate enough to give me a few minutes (out of) their busy routine and listen to my concerns. (Participant 10)
These extracts convey that compassion and care was shown towards these patients by showing that the doctors understood and responded well to their personal circumstances, paying attention to their concerns and preferences.
In contrast, other participants commented that the doctors showed inadequate compassion in their communication with them and appeared uninterested in their personal well-being. Thus, these patients felt discouraged from asking questions, and this constraint reportedly made it more difficult for them to cope with their illness:
They don’t have time to talk to patients and everything is so routine to them that they don’t have compassion towards the patient. They just ask routine questions and provide general reassurance. I am suffering so much of it without any psychological support from doctors. It is really difficult for me to cope. (Participant 19)
The doctors are not compassionate at all. They just asked a few questions about our illness but never appeared concerned with our psychological state. (Participant 21)
Two main findings emerge in relation to compassion and the doctor-patient relationship. First, there is a link made between compassion and coping (psychologically), with the implication being that an absence of compassion impacts negatively on the ability to cope. Second, the appearance of a lack of concern on the doctors’ part is recurrent within the participants’ narrative. ‘Concern’ is here distinguished from basic communication, the implication being that it is more than just asking questions, rather it requires a ‘patient-centred’ attitude that achieves a balance between meeting the patient’s clinical and psychological needs.
Expatriate doctors for whom Arabic is a second language may be hindered in expressing care and compassion by the language barrier between themselves and Saudi patients. The language barrier may mean that they appear detached from their patients and not appear as empathic, especially as they may also lack cultural sensitivity. The current study’s findings agree with previous research that indicates the positive impact of doctors’ compassion on decreasing the level of anxiety in cancer patients, which in turn increases the level of patient satisfaction and results in improved medical outcomes (Fogarty et al. 1999).
Patients’ satisfaction in an oncology setting was related to the important role that the doctor plays in all aspects of their recovery, and highlighted the need for excellent interpersonal skills in order for them to fulfil this role effectively:
To me, doctors aren’t diagnosticians only but also the ray of hope. Their behaviour, words and facial expressions are important to me, and the means by which I judge the chances of getting well. (Participant 3)
By interpersonal skills I mean the communication skills and compassion. They need to have more kindness and empathy. Here doctors are good — I don’t say they are bad — but in the situation of these skills and characteristics there is a lot lacking. (Participant 18)
A comment from one of the participants summed up the importance of the interpersonal aspects of the doctor-patient role, which appear at times to be disregarded by the medical profession, but which are often the standards by which doctors are judged by patients:
The patients classify doctors on an additional criterion that is ‘behaviour’. The doctor who’s good at his job but isn’t so supportive or caring is designated as a bad doctor, while the doctors are selected by hospitals on the basis of their abilities and experience. (Participant 3)
These findings suggest that it is not only doctors’ medical expertise that is valued but, also their interpersonal communication skills and the level of trust, compassion and ‘felt’ concern that they bring to their relationships with patients. It also suggests a disagreement between what patients value in a doctor and those attributes and values considered by doctors and important to the organisation. Non-disclosure, and language barriers may all interfere with doctor’s expression of care and may make them appear as remote figures, who show ‘detached concern’, rather than empathy. This may be a factor in patients constructing their experiences when interacting with doctors in a negative way.
5.3.2 The nurse-patient relationship
Findings in this theme can broadly be divided into two elements, which interplay to varying degrees, and show varying experiences of the nurse-patient relationship. The first of these is the sub-theme technical competence, relating to nurses’ professional skills at administering medication and other treatment. The second sub-theme is nurses’ perceived level of interpersonal skills, which are defined as encompassing a caring attitude, showing compassion, and being available to respond to patients’ needs. Beginning with an overview of participants’ overall impressions and general perception of the nurse-patient relationship, the following sections outline each of these key areas in turn, analysing their interplay.
5.3.2.1 General perceptions of the nurse-patient relationship
The majority of participants recognised the importance of the nurses’ roles and were appreciative of their help and attitudes. Those reporting positive experiences when describing their relationship with nurses used words such as ‘kindness’, ‘supportiveness’, ‘accuracy’, ‘responsiveness’, ‘trustworthiness’, and ‘understanding’, as the following extracts show:
They are always willing to help us. It’s so inspiring that despite their busy routine they like to wear a kind and reassuring smile on their faces. (Participant 13)
The nursing staff was very dedicated. They provided a great deal of help and support. They attended to each patient with a smile and performed their work diligently. They made my stay comfortable. (Participant 16)
These comments convey the impact of the nurses’ positive interpersonal attitudes (i.e. being kind and reassuring), as well as their professional qualities and competencies (performing their work diligently), on patient satisfaction.
In contrast, a few participants reported that nurses did not have supportive attitudes, and were sometimes too busy for positive communication. The most noteworthy aspects of dissatisfaction related to issues such as inadequate attention to individual patients’ needs and a lack of psychological support:
Generally, nurses are good but need to recognise the psychological status of the patient by allowing more time to spend with cancer patients when asking questions. (Participant 5)
The nursing staff is good but there’s a lot of need for further development. They are not able to adapt to patients of different mind-sets, having a generalised attitude which isn’t sufficient at all. And that’s the reason I’m not really satisfied. (Participant 7)
The findings also indicate that, in order to deliver improvements regarding the nurse-patient relationship, there is a need to address organisational constraints. These include the low number of trained nurses at the hospital, which places a strain on their capacity and/or capability. It seems that there is a need to increase the number of nurses and enhance their efficiency so that they can devote more time to effective communication with their patients, as illustrated by the responses of two participants:-
They are good but they are very busy and there is a real staff shortage. (Participant 1)
The number of nurses is a drawback, as they are limited. Therefore, sometimes I don’t want to bother them to get assistance for the bathroom, so I asked them to teach me how to disconnect the IV plug, and then it was easier for me to help myself. But of course, when I need them they are around and respond well to my calls. (Participant 18)
The last excerpt highlights the awareness that, while nurses’ capacity may be limited, this is not owing to any technical incompetency or lack of care, but is rather an issue of resources. The positive opinions towards the end of the extract indicate that, despite constraints, nurses do make themselves available to help patients with urgent needs. However, some of participants mentioned a lack of psychological support rather than technical assistance as being the key feature that defined their relationship with nurses:
Nurses need to be specifically trained to deal with cancer patients. They should be aware of our psychological state and their attitude should provide confidence to patients as we sometimes have many questions or are worried about the next appointment or discharge. They should welcome questions and comfort us with patience and kindness. (Participant 21)
This extract gives the impression that the nurses did not fulfil their role appropriately and failed to offer psychological support, which is important for a patient-centred approach to nursing. Moreover this participant felt that nurses should focus more on communication and relationship building. Overall, it was apparent that a nurse not having sufficient time to interact and communicate with patients was a determinant of patient satisfaction with the nurse/patient relationship. These findings concur with those of Shattell (2004) and Rachiadia (2009), who indicate that patients want nurses who are approachable, available, empathic and willing to talk with them, as well as nurses who are not rushed because of their workload and responsibilities.
5.3.2.2 Nurses’ technical skills
Having confidence in professionals’ technical competence represents one of the most important underlying indicators of patient satisfaction or dissatisfaction with nursing care (Dowling 2008; Wagner and Bear 2009; Zhao et al. 2009). The findings indicate that patients generally have positive attitudes towards nurses’ technical skills. Most of the participants highlighted the proficiency of nurses’ professional and technical competence, also asserting that such competence helped to build trust between them and the nurses. A recurrent notion that was also seen to be important in the doctor-patient relationship, was “trust” built on patients’ perception of nurses’ expertise:
Nurses are with us all day round. Their technical expertise in preparing accurate drugs, administering them properly at the right pace and constantly watching for any alarming symptoms, are vital for any patient. I am happy that the nursing staff attending to me were all expert in their profession and I did not face any trouble during my stay. (Participant 16)
Their time management and team work impressed me a lot. They were overburdened yet they managed to deliver the correct drug at the correct time to all the patients. They were well organised and very professional in their job. (Participant 17)
The nurses were very professional and have good experience. They took enough care to be accurate with indicated treatment. Whenever they had a doubt they consulted the doctor to be accurate. I am impressed with their competence. (Participant 15)
These comments reveal a high level of satisfaction with the attendant nurses, which in turn had a positive influence on patients’ constructions of their interactions with nurses.
In contrast, some participants had less positive experiences, in particular voicing uncertainty or concerns over the technical expertise of some nurses. There was often an apparent lack of understanding regarding the nature of the chemotherapy treatment being administered and anxiety over the accuracy of its administration. Such concerns could stem from the fact that the ultimate objective of these patients was to cure their cancer and survive the illness, which depends directly upon the technical skills of the nurses supporting them. The following are examples of these experiences; that is, of problems arising from a deficit in nurses’ skills or knowledge:
In my first visit a nurse had almost given me the very strong tablets intended for my neighbouring patient. But fortunately she realised her mistake in time and I threw up the medicine. Since then I keep a keen eye on my medication. (Participant 6)
Medication administration seems the most important technical skill to me. Nurses should consider the medications they control for patients. They work so closely with patients that they are for the most part the ones who capture drug slips made either by the pharmacist or prescribing doctor. Drug handling is important as well. (Participant 6)
Some participants made several constructive suggestions regarding what could be done to improve the relationship between patient and nurse and implying that more could be done to make their experiences more satisfying in an oncology setting. Examples of possible improvements in the patient-nurse include better time management, better explanation of medication administration and, in particular, enhanced skills at inserting intravenous lines. It was also emphasised that nurses should be better trained to ensure the optimal skills in intravenous therapy, as one participant states:
Hate anaesthesia, it makes me feel very uncomfortable. And it feels even worse if the nurses have to try 2 or 3 times to insert the medication. I wish that nurses could learn to do it and get well trained at it so they would be able to do it with one attempt. (Participant 13)
Researchers argue that patients often view optimum nursing care as a combination of practical skills and professional knowledge, which are agreed as fundamental to all nursing practice (Halldorsdottir and Hamrin 1997; Calman 2006; Duff 2013). From a nursing perspective, competence has been defined by ICN (2005, p. 6) as ‘the effective application of a combination of knowledge, skill and judgment demonstrated by an individual in daily practice or job performance’. Specifically, in terms of nursing definitions, competence reflects the following: knowledge, understanding, and judgment; a range of skills, including cognitive, technical, or psychomotor and interpersonal; and a range of interpersonal attributes and attitudes (ICN 2005). This definition describes a fundamental requirement which influences the quality of care of the participants. The findings of the current studythe current study suggest that there is a need to address nursing competencies, especially in relation to medication administration and the insertion of intravenous lines for chemotherapy.
5.3.2.3 Nurses’ interpersonal skills
Participants mentioned several aspect of nurses’ interpersonal skills as significant: 1) being caring, supportive and compassionate; 2) paying attention to the patients’ psychological as well as medical needs; 3) responding appropriately and taking time to listen and understand the patients’ needs; and 4) ensuring they are available whenever patients need them, even when overloaded with work. By embracing all of these, the nurse-patient relationship was seen to have the potential to evolve into a trusting relationship.
5.3.2.4 Care and compassion
Participants generally felt that nurses should be able to understand patients’ needs. Some vital interpersonal skills that were highlighted related to the level of nurses’ supportiveness, care and compassion. A connection was apparent between the levels of care and compassion shown by nurses and the motivation of patients to get better, which, in turn, related to patients’ level of satisfaction with their care:
They spent time talking with me. I found it so lovely and caring and sensitive to my needs, I really appreciate them and their way of dealing and sharing with patients. I see this as very important to cancer patients, to be surrounded by good nurses who are willing to accept and talk and dedicate their time to us. (Participant 8)
They were caring towards me... Their kindness and sympathetic attitude were always encouraging and helped me to cope during my stay, thank God… They always asked me if I had any complaints or if I needed pain medication. Even if I rang them they were quick to respond and provide me with comfort and help during either their day or night shift. (Participant 20)
In contrast, other participants reported negative aspects of their interpersonal relationship with the nurses, including inadequate attention to the individual patient’s needs and a perceived lack of understanding and failure to supply support. There are several possible reasons for this, including the work load of the nurses. The non-disclosure issue may influence nurses’ attitudes to communicating with patients. They may interpret the non-disclosure requirements of some families as meaning that they must avoid their communications with all patients or they may seek to minimise communication to avoid patients, especially female patients from asking questions, which the nurses are prohibited from answering. This will mean that patients build their interactions with nurses as being unsatisfactory.
Some participants also noted that nurses did not always have enough time to give patients adequate attention. This was complicated by the fact that some of the nurses were non-Saudi nationals, for whom Arabic was a second language:
Generally, the nurses are good but need to recognise the patient’s psychological state by allowing more time to spend with cancer patients when asking questions. They should also ask for a translator if the patient can’t understand some points in conversations, such as helping with room transfer from a shared to a single room. (Participant 5)
This again raises the issue of resources of time and cost for translation, specifically, the challenge of expatriate nurses, who potentially do not have adequate capacity to develop trust and good communication with patients. This may also be due to a lack of proper language training, specifically Arabic. Previous research indicates that, without a shared culture and language, it is difficult for expatriate nurses to deliver effective nursing care to Saudis (Al-Shahri 2002; Al-Dossary 2008). The language barrier may lead nurses to appear as detached and remote to the patients. This is contrary to the patients’ expectations of how a nurse should behave and act (Rchaidia et al. 2009). Such barriers will lead to patients construing their experiences with some nurses, as being unsatisfactory.
The finding discussed in this section have shown the importance of nurses being perceived as compassionate and caring by patients, features that have been highlighted in cross-cultural studies. For example, a review by Rchaidia et al. (2009), who investigated cancer patients’ perceptions of the ‘good nurse’, indicates that the personal characteristics of being caring, showing compassion and relating to the patient as a person are fundamental traits, which pertain to both western and eastern cultures. My findings would suggest (as in the case of the doctors) that cultural attitudes and the language barrier may interfere with nurses’ ability to express empathy and care that is expected of them by patients. If nurses are perceived as not acting compassionately and expressing care then they are not acting in ways that a patient can construe as appropriate or satisfying.
5.3.2.5 Availability: ‘Being present’
The findings demonstrate that several participants had a positive attitude towards nurses’ availability and their time management during care provision:
Their time management is commendable. They attended each patient with great competence. They performed their duties… dedicated enough time to each patient. (Participant 15)
However, other participants noted that nurses were sometimes too busy to give patients the attention they needed:
They just need more time to spend with patients as they have a staff shortage and the nurse couldn’t spend time with me when I asked or called in the afternoon... Then they do attend… but they just need to be faster… one nurse who was caring for me had two beds in the room to look after so I always felt too shy to ask her for help with walking or the bathroom as I could see she was busy and couldn’t help me. (Participant 5)
The emphasis was on nurses being present and devoting the appropriate amount of attention predominantly to patients’ physical needs, but also to psychological needs, since the right attitude can make patients feel more comfortable. According to Rchaidia et al. (2009), this state of ‘being present’ both physically and mentally in terms of their openness to patients’ psychological needs, is an important indicator of a good nurse, based on the perceptions of cancer patients.
5.3.3 Contextual factors relevant to cancer in the KSA
The third theme which is contextual factors seen as specific to the context of cancer in the KSA, also emerged as important to patients’ perceptions of treatment and the level of care being provided. The subthemes of the contextual factors that found are: the patient perception of cancer, culturally endorsed power dynamics regarding the doctor-patient relationship, the influence of religion, the role of family, and the effects of a multi-cultural hospital environment. The next section presents findings from the analysis of interview data regarding these subthemes that emerged from the current study. This facilitates identification of key factors relating to the KSA cancer context.
5.3.3.1 Patients’ perceptions of cancer
Patients within the KSA view certain illnesses, such as cancer, as being of greater medical priority than other forms of disease or illness. Therefore, oncology patients believe they are deserving of greater attention from medical staff and require better treatment conditions. The following quotes illustrate this:
Yes, oncology patients must have priority in appointments for labs or x-ray. (Participant 8)
Organisations should learn to treat cancer patients differently to other patients. They should understand that time is of utmost importance in our treatment. Any delay on their part could have a devastating impact. They could help us a lot by improving the pace of functioning. (Participant 1)
These extracts convey some participants’ perceptions that oncology patients should be given priority in accordance with their special requirements. The second extract, in particular, emphasises the urgency with which the need for treatment is perceived, with words such as ‘priority’, ‘delay’, and ‘pace’ in both extracts denoting the importance of timeliness.
Illness, particularly cancer, is perceived in various ways depending on national or regional cultural factors. In the context of the current study, participants’ perceptions that cancer should have priority status in terms of treatment may be drawn from the cultural beliefs of the KSA that cancer is likely to be an imminent death sentence. For example, one participant commented:
I never knew about cancer and its treatment. In my mind it was just one fatal disease and I knew nothing else about it. But when I came here and the tests confirmed that I had cancer, I started believing that I would be dead in few days. (Participant 12)
Similarly, cancer has been found to carry a social stigma worldwide (Goffman 1963; Albrecht et al. 1982; Chapple et al. 2004; Rosman 2004). However, Joffe (2002) has argued that fear of cancer has decreased markedly as medical knowledge and success rates have increased. Nevertheless, the my findings indicate that cancer within the KSA is perceived in ways that go beyond stigma alone; that is, as a fatal disease which can evoke a strong fear of death.
Another factor that has been found in other studies to impact on oncology patients’ satisfaction is the treatment environment (Gotlieb 2000; Ulrich et al. 2004; Rowlands and Noble 2008). Related evidence has emerged in the current study, where patients’ main concern was not being able to have privacy. The following participants emphasised the importance of having a single room, as being in a shared arrangement adversely affected them physically and psychologically:
I feel so shy when I have nausea in a shared room as I can’t tolerate the smells of food during lunch time. That’s why I am so irritated at sharing a room with someone. But if I am in a single room, I feel comfortable and free to request from the nurse that no food should be supplied to my room due to my severe nausea. (Participant 3)
Having a single room is important for me because I feel comfortable when I can sleep and rest with no noise, and can have a quiet place to rest and read the Quran. I prefer to be alone and not to socialise with people during my stay as staying with people increases my worries and fear as other patient have different treatment and stages, which is not always encouraging to me. (Participant 5)
For example, high-quality environments with high levels of support seem to be associated with higher levels of patient satisfaction, especially for the most severely compromised patients (Timko and Moos 1998a). The findings of the current study also demonstrate the importance of a treatment environment that is sensitive to oncology patients’ needs, particularly the need to be able to express the physical symptoms of their illness without fear of shame or embarrassment. Being unable to do so has a negative psychological effect and may even make patients feel uncared for and despondent over whether they will get better, as the extracts illustrate. A central desire was for a private space if they were very ill. These findings indicate that patient preferences are deemed to be an important element in providing patient-centred care, thus influencing the level of cancer patient satisfaction.
As these findings have shown, patients’ perceptions of cancer specifically in the KSA context, and their experience of the treatment environment both contribute to their perception of the treatment they should be receiving, and the quality of actual care they feel they are receiving. The following sections elaborate on the other key contextual factors affecting this perception.
5.3.3.2 The influence of doctor-patient power dynamics
As shown in section 2.5.2.4 in chapter 2 and section 5.3.1 of chapter 5, the doctor-patient relationship in the KSA context is typically mediated by the perception of doctors being powerful figures of authority whose word should be trusted, rather than encouraging dialogue or discussion between doctor and patient for purposes of shared decision-making.
Patients’ perceptions of doctors in the KSA, and the power imbalance that occurs, can be seen as closely related to the conventional role of physicians in KSA culture. Whether or not they are native to the KSA, doctors are considered to be highly respected figures of authority (Elzubier 2002). As one respondent commented:-
The relationship with doctors is important to every patient. We actually give them, after God, the authority over our body and illness, so having a good trusting relationship with my doctors keeps me calm and satisfied. (Participant 9)
Doctors are positioned as the ultimate human authority on health, who, by implication, have the necessary knowledge and skills to administer whatever treatment is best for the patient, and therefore should not be questioned. This view, in turn, lends itself to a top-down power relationship between some patients and their doctors, as the following extracts illustrate:
The doctors were not interested in patients’ mental condition. They took care of treatment and that’s it. We could not feel comfortable enough to express our concerns to them. This has adversely affected the whole situation by making us feel unmotivated. (Participant 19)
In the beginning, I had endless fears and doubts but I wasn’t able to talk about it with my doctors. I had once tried to tell them about it but they shooed me away and since then I never gathered enough courage to communicate openly with them. (Participant 7)
Both of these extracts imply a sense of being intimidated or ‘not comfortable’ with doctors. In particular, the fact that the second participant’s anxiety is not adequately listened to and the necessary knowledge is not shared highlights an unequal balance of power and control in the patient-doctor relationship. Participant seven’s emphasis on (lack of) ‘courage’ suggests a state of feeling intimidated by those who have the power to allay the fears and doubts associated with the illness. The participant’s feelings may stem from the fact that families wish to restrict information, a cultural attitude. This means that patients can feel anxious because they have little or no information on their treatment keeping them in the dark and questioning the treatment options chosen for them. The anxious feeling and the feeling of being shut out of making decisions of their own body leads to their dissatisfaction of the healthcare provided to them. Patients such as participant seven desire to overcome the family restrictions that are placed on them terms of their treatment and giving them the sole right to decide about their healthcare.
In contrast, several patients mentioned feeling very well-informed by doctors, to the extent of feeling they knew whether their illness would be cured or not. Given the strong cultural context at work, this effect can be seen as part of the high regard in which doctors are held in the KSA. As one respondent stated:
The doctors in oncology were so respectful and helpful, they tell me everything about my condition and options for treatment such as surgery, chemo and radiation, also they were honest about prognosis and this was so important for me to know (whether my disease is) curable or not. (Participant 8)
This finding also reflects a cultural shift in doctors’ information provision to patients in the KSA as evident from the experience of the participants in the current study, indicating that they are increasingly providing patients with full details about their condition, such as the prognosis.
As discussed in chapter 2, studies conducted in the KSA and internationally (Al-Ahwal 1998; Tanaka et al. 1999; Al-Amri 2010) provide evidence that patients prefer to have full disclosure of information about their illnesses. In contrast, surveys of physicians in the KSA (Bedikian et al. 1985; Mobeireek et al. 1996) have revealed their preference for discussing patients’ condition and treatment with patients’ close relatives rather than with the patients themselves. More recently, however, there has been growing public awareness of medical issues, as well as ethical pressures, in the KSA that are reportedly driving a change in doctors’ attitudes and behaviour, with full disclosure of diagnosis to the patient rather than their relatives becoming more common (Sokol 2006; Mobeireek et al. 2008; Al-Amri 2010; Aljubran 2010). The current study’s findings support that doctors in the KSA today provide full disclosure of information to oncology patients which implies that it has become a norm, however, if the family has expressly stated that a patient is not to be informed of about their health or treatment doctors do not do so.
Considering these cultural factors, it becomes evident that the perceived power imbalance between doctors and patients can affect patient satisfaction with care either positively or negatively, depending largely on the interpersonal dimension, that is, the capacity and the way in which doctors deliver the relevant information. Some of the participants indicated the ideal power balance they would like to have with doctors, including a preference for an open and trusting relationship in which they could feel comfortable discussing any of their concerns in a sensitive manner. The following extracts illustrate these expectations:
A patient should trust and be able to depend on his doctor. This relationship develops with understanding and interaction. Doctors shouldn’t be the medicine/treatment prescribers but also a counsellor. (Participant 21)
The personal skills of the doctors here need much improvement as they should consider the psychological state of the cancer patient. I want them to deal with me in a kind way and consider that their attitude will affect the patient, like if they didn’t listen or just try to be in hurry during visits. (Participant 7)
This apparent change of attitude where patients wish to build relationships of trust with their doctors and openly verbalise their concerns is surprising in a KSA context. This preference for patient empowerment and advocacy is arguably at variance with cultural norms in the KSA. These patients’ attitudes, and their emphasis on doctors’ ‘kindness’, represent a shift towards the need for a more western and patient-centred approach involving active patient participation in care.
5.3.3.4 The influence of religion
In the current study, a major point to consider was that the religion of Islam is the main aspect shaping the culture of the KSA. Many of the participants indicated that their faith affected their perceptions not only of their disease, but also of the care they received. These findings add to other studies conducted in KSA which have drawn the importance of faith in receiving healthcare, particularly the study conducted by Halligan (2006) who argues that Islam is a contributing influence on patient satisfaction. He highlights the way in which the influence of Islam can be felt in every aspect of patient care. All of the participants in Halligan’s study, who were expatriate nurses, recounted that everything people do is centred on religion, and it is the main way of life. Consequently, Halligan (2006) correlates patients’ attitudes towards their illness with their religion, which is identified as ‘central to the provision of caring’ (Halligan 2006 p1565). The current study adds to the discussion produced by Halligan (2006) as it brings to surface the impact of religion on patient’s assessment of healthcare delivery while Halligan (2006) focused on experiences of nurses.
In the current study, participants indicated that their belief in God was more powerful than medicine. In addition, some of the participants stated that it is their faith and connection with God through prayer that helps to keep their spirits up, as one person stated:
I believe that my disease has been gifted from God as a test to see how I will be patient and deal with this fact; therefore, I accept my destiny of cancer and I will be working hard to deal with recovery by praying first to God to help me and then also to help my doctors to cure my disease in the near future, Inshallah. (Participant 8)
These finding are in line with other research which conveys the positive influence of religion on coping with cancer; specifically, some have argued that cancer patients in Islamic countries have better coping mechanisms than those in other countries (Ezzat et al. 1995; Young et al. 1997; Silbermann and Hassan 2011). The current study uses patients directly as participants and adds to other research which used doctors or nurses to assess the impact on faith as a coping mechanism when dealing with cancer.
The emphasis on the spiritual dimension of coping in illness was also evident through the fact that SRCCs have visiting religious scholars, who are on hand to lend patients moral support and spiritual guidance through their situation, and some of the participants commented on this aspect of their care:
The weekly official visit of a religious scholar was very helpful and motivating for me and other patients. I felt so great during religious scholar visits and really need the hospital to consider his visits to be daily for patients, as this reassured me and helped me a lot in my spiritual condition during the treatment. When I felt lost I wished to see someone who could connect my heart with God so I could find some peace. (Participant 7)
Religious lectures on Islamic affairs are needed to bring positive changes for us as cancer patients. (Participant 12)
These extracts demonstrate the importance placed on spiritual health by these oncology patients, and highlights how a visit by a religious counsellor or a lecturer on religious themes can fulfil the spiritual needs of the patients. This fulfilment is also shown to improve their mood and confidence about their situation, as conveyed through language such as attaining ‘peace’ and ‘positive changes’.
However, other participants presented contrasting views by emphasising their belief that the doctors and nurses were the only ones who could help them:
I believe that they are the only ones who could clear my mind about my situation. (Participant 10)
This extract echoes the other dominant cultural context that is relevant here, that is, the conventional perception of physicians in the KSA, who are seen as highly respected figures of authority (Elzubier 2002).
5.3.3.5 The influence of family
The principal idea of family is fundamental to the provision of care within the KSA. This is further supported by Halligan (2006) and Younge et al. (1997), who argue that the importance of family has a direct impact on the perceived level of care by the patient. This is especially the case with the family’s ability to influence doctors’ disclosure of information to a patient. These researchers describe family involvement as pivotal to the experience of the care being delivered and as a significant factor affecting the emotional, social, and psychological well-being of the patient.
In the context of the current study, family members were viewed as the principal decision-makers who often dictate the care that patients receive, including the extent of the care to be given. For example, participants in the current study recounted both how families help to direct their treatment and also offer vital moral support:
Thank God my family are with me; this helps me bear the after effects of the treatment. (Participant 21)
However, while the patient’s family has significant influence on the care to be provided, patients still look to the medical staff, such as their doctor, for ultimate guidance and explanation of treatment prior to making any decisions. In the following extracts, participants underline the doctors’ involvement in the process of informing family members as well as the patient him/herself:
But my mother wasn’t able to understand and she was very afraid. The doctors calmed her down and assured her that they wouldn’t be doing anything wrong to me. (Participant 13)
They explained all about the treatment to my husband. (Participant 22)
These extracts underline the critical role of the family, in that they are physically present at key diagnostic stages; the implication here is that they are then expected to be involved in subsequent decision-making about treatment. This is in line with other findings that, in developed countries, patients often demand more resources, i.e. medical staff attention, to be available to their family (Given et al. 2001). However, these extracts also emphasise the continuing importance of medical staff not only for informing and reassuring the patient, but also for reassuring all members of the family. Thus, while the family can be a determining factor in terms of care, patients are also aware that professionally trained medical staff are essential in providing clarification and ultimately informing treatment decisions (Given et al. 2001; Ezubair 2002).
However, the influence of family, although fundamental is still bias towards females. As noted before, female patients in KSA need the presence of male guardians which can be their father, husband, or son depending on their marital status. The treatment decisions of female patients fall on the father or brother if she is unmarried, on the husband if married, or on the son if widowed or divorced with children. This contrasts to the role that women have when the patient is male. The treatment decision making, disclosure of information, and advise given by a doctor or nurse in the case of male patient is restricted to the male members of the family. In the case of a male patient, the wife is not the sole decision maker for her husband, the male family members of the patient are the ones who are handed the responsibility of decision making and being the main point of contact for information. This is due to the societal hierarchy framed from cultural beliefs within KSA which is male-centric and male dominated.
5.3.3.6 The influence of the multi-cultural health care environment
The health care environment and its own cultural context play a vital role in patient satisfaction (Rafii et al., 2008). A major cultural factor in terms of the KSA hospital environment, and prevalent in the specific SRCC examined in the current study, is the presence of largely expatriate nursing and medical staff from all over the world (in particular South Africa, India and the Philippines) who are unlikely to speak Arabic (Luna 1998; Al-Dossary 2008). In particular, the expatriate nursing staff were found to affect patient satisfaction in that their difficulties with the Arabic language created some tension in communicating with patients. Many participants noted that they could only express their emotions and needs clearly in Arabic languages, which these nurses were not always able to understand fully. As several participants commented:
Their language is a bit of problem; it would be easier to communicate with them if they were capable of speaking Arabic. (Participant 10)
Communication skills are the most important, for example, being able to talk freely and ask about treatment, but in my opinion the nurses need to understand more of the Arabic language to be able to deal with patients easily. (Participant 5)
Inadequate communication arising from language barriers can be seen as a determinant of these patients’ satisfaction level, frequently causing a loss of rapport with nurses. Accordingly, Arabic-speaking nurses were deemed more likely to provide the optimum psychological support and to be able to meet patients’ medical needs than non-Arabic speakers. Evidence of language barriers in communication between the patient and their nurses has been reported by a number of studies in the KSA owing to these nurses frequently being non-KSA nationals (Al-Shahri 2002; Attalah et al. 2013). As previously mentioned, there is, however, currently a drive towards employing greater numbers of Saudi Arabian nurses or Arabic national nurses as part of the Saudisation process (Al-Malki et al. 2011).
Because of the multi-national mix of personnel, including many non-Saudi doctors, English was the default language being spoken among professionals in the presence of the patient, and this could create a feeling of anxiety in the patients. The following extract illustrates this:
For example, the doctor saw me and requested some tests or radiology; then I asked the nurse, but she said there was no instruction written by doctors, so I felt lost between doctors and nurses because doctors speak English with them in front of me, which is difficult for me to understand – is he requesting something or just talking? That’s why I felt worried and asked a lot if doctors were requesting tests or x-rays. (Participant 5)
In this patient’s case, the language barrier negatively affected the way patient constructed their experiences. The use of English rather than Arabic by the medical staff led the patient to feel excluded from discussions about his/her own health, and created a sense of dissatisfaction with the care they were receiving. The issue of the language barrier here overlapped with the requirement of non-disclosure to the patient, thus compounding the potential problems with establishing a personal relationship between expatriate nurses and Saudi patients.
Personal relationships can only be established when communications are possible. The fact that a nurse and patient only have limited communications mean that a nurse can appear as not engaging with a patient or may appear as being inattentive. The ability of a nurse to establish a relationship is further impacted by the fact that they often have to ensure that they don’t disclose information to a patient at the request of the family which is considered a norm of non-disclosure in the KSA healthcare setting. This may make nurses unwilling to spend time and interact with a patient. The language barrier and non-disclosure means that often the nurse-patient relationship is not a satisfying one for both parties.
Language barriers must be addressed in order to ensure quality trans-cultural nursing, given the high proportion of expatriate, non-Arabic speakers in the KSA (Luna 1998; Al-Shahri 2002). It can be argued that the gap, identified here and in previous studies, between patient needs and the language barriers of expatriate nurses may adversely affect the degree of care provided, thus lowering patient satisfaction levels (Al-Shahri 2002; Ezubair 2002; Al-Dossary 2008).
This section has highlighted the importance of nurses and other medical staff in oncology wards tailoring their care to patients’ needs and providing a more patient-centred approach, as this can significantly affect patient satisfaction levels.
5.3.4 Organisational factors impacting patient care
This section presents the findings from the study that highlights the organisational factors influencing patients’ satisfaction or dissatisfaction. Based on the participants’ responses, three main factors were identified as important aspects of the service organisation which influenced their overall satisfaction levels: (1) accessibility to healthcare (i.e. having full access to the hospital and permission to use all the necessary facilities); (2) general service organisation and (3) waiting times (i.e. that they should be reasonable and that the staff should be supportive of patients while they were awaiting treatment).
Prior to a more detailed examination of each of these factors, patients’ perceptions of the general service organisation are detailed in the next section. This is followed by a presentation of the findings relating to each of the three key organisational factors.
5.3.4.1 Perceptions of general service organisation
Overall, there was a mix of views among the research participants regarding their experiences of the service organisation, with many indicating that, while they were generally happy, there was some dissatisfaction with the operational structure of the facility.
The majority of participants who reported positive feedback on the general service organisation talked about both the medical services and overall service organisation:
The referral system is good here. Labs and other testing services are very good and prompt. I don’t have any problem with them. (Participant 9)
My overall experience with the service organisation during my stay is good. (Participant 4)
In particular, some of the participants emphasised the high level of effectiveness of cancer support services with regard to the non-medical support they received, including that provided by the social workers:
I wish them all the best as this main referral hospital deals with a large number of patients and still manages to have great services available to us, such as a social worker and Saudi cancer society officer, who always support me. (Participant 16)
I have the ability to connect freely to the Internet during my stay, as well as social worker services that let me feel happy and rest assured. Also the way they approach me is friendly and helps me feel supported and satisfied during my hospital stay. (Participant 8)
However, some of the participants reported negative experiences of the organisation of medical services. The following extract illustrates this factor:
I had to wait for a long time to obtain the approval of referrals. My treatment was delayed because of a delay at the lab. Sometimes it was really troublesome to get things done with them. (Participant 19)
The previous extract highlights one of the most problematic issues, as several participants reported long waiting times for referrals, admission and for labs. The waiting time for psychiatric services was also seen as problematic:
Other services like referral took a long time, it took a long time to get appointments and it was very uncomfortable to be seen by psychiatric services after 1 month. Generally, I don’t like this waiting time because I feel more worried and less assured, which sometimes makes me feel unstable and anxious during my stay. (Participant 3)
These findings demonstrate that, while there are positive findings regarding the healthcare services, there may be a need to improve certain aspects of service provision for oncology patients, particularly with regard to waiting times and doctor availability. The following interview excerpts emphasise this point:
It’s worrisome and irritating to wait so long. Especially for cancer patients, it’s even more irritating to wait. I don’t like it when hospital management forget about the psychological state of their patients. (Participant 13)
What is needed is making more doctors available to oncology patients. (Participant 3)
The opinions arising from these excerpts and discussed throughout this section show that there are several organisational policy factors that may be at odds with patients’ preferences for the treatment setting or logistics of care such as referrals that are not seen as fast enough and a shortage of medical staff on oncology wards.
5.4.4.2 Accessibility to health care
Participants in the current study reported positive experiences regarding access:
It was good and I didn’t face any problems with it as it was well arranged. There were always supportive services, for example from the social worker or from the cancer support society. (Participant 20)
The admission process was good, well ordered. I didn’t have problem in waiting for admission or referral; it was perfect during my stay. (Participant 8)
In contrast to these positive experiences, some reported several problems with accessing the hospital and its facilities; the following is an example:
I remember the trouble I had to bear at my first CT scan. Firstly, it was crowded all the time and the personnel didn’t bother to do things quickly. I had to wait for two hours to get it done. According to them, it was a busy day, but I think if it’s better organised or there is a separate clinic for oncology it would benefit us more and improve our experiences. Also, referrals and labs have been working at a poor pace. My referral to an orthopaedist took three months; I was already on pain medication but still looking to see a specialist as soon as possible to get a clearer idea about the knee pain. (Participant 18)
Sometimes I got correct information but most of the time it was very confusing. There is lack of coordination between departments and nobody is in a position to provide all the information. The people here were also unconcerned with the trouble of the patient. (Participant 19)
These negative experiences relate mainly to the slow pace at which care was given, and the lack of coordination in information giving or confusion regarding the information actually provided. Timeliness was closely linked with efficient access to services, and impacted adversely on patients’ satisfaction if it was not present. In addition, patients’ criticism of crowded circumstances also denotes the importance of the hospital environment when accessing it, which the following section explores in further detail.
5.4.4.3 Waiting times for services
Waiting times are one of the indicators that have been found to influence patients’ perceptions of the health care service and lead them to construct their experiences with it as satisfactory. In the current study, the waiting times for services were mainly positively assessed by the participants, as these extracts show:
I had a very good experience with the service of the organisation during my stay. There was well organised admission in a timely manner, and that was excellent. (Participant 16)
I feel so comfortable and like the earlier arrangement, such as getting my blood test earlier before going to the admissions office, which means that I can process my admission after the oncology staff confirmation, so that is very well arranged and organised and then I will just be waiting for doctors to be seen directly and treatment to be started. (Participant 8)
In contrast to these positive experiences, some reported that usually admission took longer and they had to spend time waiting in the emergency room for oncology doctors to decide and agree about admission. If patients book ahead for the admission process, it becomes easier and means that they can reach the doctor easily without a further waiting period. The following extracts demonstrate several patients’ dissatisfaction with admission and referral times:
I have been referred to two different doctors – a psychologist and neurologist – and neither of them have any available appointments; it has been almost a month now. It has been really hard for me to wait for so long. (Participant 11)
My admission had been delayed for 8 days. Isn’t this unfair and troubling? And the reason behind it is the unavailability of beds in oncology wards. I couldn’t be admitted to any other wards in hospital to receive my scheduled treatment. (Participant 6)
By using language such as ‘unfair’, ‘really hard’, and ‘troubling’, these participants display a feeling of neglect that is experienced by patients being left to wait for long periods of time for medical attention and referrals, in some cases to the extent that they need to seek private care. This feeling of neglect can also be seen as connected to patients’ views that cancer is a priority disorder. Similarly, other professionals have argued that inadequate access to KSA cancer services such as the long waiting times negatively affects the level of patient satisfaction with the care provided (Al-Muziani 1998; Al-Sirafy 2009).
In light of this, another important element to assess is the perceived level of supportiveness of the health care personnel during these waiting times. Participants mainly reported positive experiences, emphasising the staff’s supportiveness, helpfulness and willingness to help:
Whomever I interacted with, they were well informed, nice and patient. They always provided us with the correct information about the services. (Participant 17)
They are cooperative and helpful in guiding me if I need help such as fixing an appointment or changing the time of an appointment; they have been very cooperative with this. (Participant 8)
However, others noted less positive impressions of their communication with the medical staff during the time they were waiting to receive medical help:
They are good but CT staff need to be more kind and patient, especially with oncology patients. Lab services are usually crowded and need more organisation to make sure they have enough space to accommodate all the patients and not have them always waiting in corridors for a lab call as it's not helpful for patients to be in crowds with their pain. (Participant 3)
Another thing is the lack of psychological understanding among medical staff. They don’t try to understand the patient’s individual psyche. (Participant 6)
These criticisms indicate that medical staff need to act kinder and provide more supportive care, especially towards oncology patients, and that they sometimes demonstrate an inadequate psychological understanding of their patients’ needs.
As the following extracts also show, reference to crowded space and a lack of proper organisation indicates that participants felt that having adequate coordination within the health care system was important, yet was perceived as currently problematic and impacting on waiting times. This is illustrated by one who stated:
There is lack of coordination between departments and nobody is in a position to provide all the information. For example, my next readmission date was not provided until after discharge as the clerk was unavailable that day, so we had to follow this up with them after discharge and my son had to go back to get it confirmed. (Participant 21)
Another connected the problem of long waiting times with the shortage of nurses and the approachability of available staff noting that:
Here the situation is dependent upon the individual personnel; some of them are willing to help and some aren’t. No, I can’t reach out to all personnel if I need, they don’t seem easy going. (Participant 10)
The issues of capacity and problems with staff shortages have been highlighted by some researchers attempting to elucidate the impact of the staffing levels of nurses and the mix of nursing personnel in hospitals on patient satisfaction. For example, one study argues that hospital administrators, accrediting agencies, insurers, and regulators should take action to ensure that adequate nursing staff are available to protect patients and to improve the quality of care (Needleman and Buerhaus 2002). The current study found that good accessibility to health care – in terms of waiting times and availability of oncology ward staff (doctors, nurses) – are important factors influencing patient satisfaction in the KSA.
- Non-disclosure in the KSA setting
5.5 Summary of key qualitative findings
The qualitative phase of the current study has explored the ways in which interpersonal aspects of care and accessibility to health care influence patient satisfaction in an oncology ward setting at the SRCC in Riyadh. It has considered the role of cultural and organisational factors relevant to the health care context, as well as within the wider KSA society, in influencing these satisfaction levels. Four key themes have been identified and explored: (1) the doctor-patient relationship, (2) the nurse-patient relationship, (3) contextual factors relevant to cancer in the KSA, and (4) organisational factors.
A strong emphasis on the psychological as well as physical elements of care was evident; with many patients highlighting that doctor should understand and respond well to psychological state. Nurses’ interpersonal skills were deemed important and impacts on the quality of their experience. Largely, nurses were seen as supportive and understanding. However, some patients perceived the nurses as lacking in compassion and responsiveness, although this was also linked with nursing shortages and the observed lack of time that nurses had to interact with patients. In addition, it is attributable to the non-disclosure policies variability that instructs some nurses not to communicate certain health information to patients.
In relation to KSA contextual factors, it is evident that cultural perceptions of the doctor as a figure of authority and power in relation to one’s health often engendered a top-down power dynamic, where patients felt constrained about asking questions or interacting with doctors. However, other patients recognised the need for a more balanced dynamic of trust and rapport. In addition, there was evidence to suggest doctors are increasingly sharing information with patients themselves rather than with their families, as has historically been the norm in KSA. This departure from longstanding non-disclosure policies appears to promote patient satisfaction.
The multicultural care environment, comprising mainly expatriate nurses, had an impact on patient satisfaction levels. The language barrier with nurses who did not speak Arabic presented challenges to some patients and lowered their satisfaction with nursing care. In addition, the default English-speaking between doctors and nurses engendered a feeling of exclusion and anxiety among some patients.
The findings were mixed relating to patients’ perceptions of the SRCC’s operational efficiency and its impact on their satisfaction with care. While some participants praised the SRCC for its efficiency, environment and admission processes, many voiced strong views in their criticism of two main organisational factors: accessibility to health care and waiting times. These two factors were closely linked. Many patients noted having had to wait for long periods of time to be admitted to hospital, whether for a referral, or to gain access to a laboratory test or results. This, in turn, compromised their access to the treatment they needed and greatly lowered their levels of satisfaction with the services offered.
The norm of non-disclosure was considered a common factor that influenced patient satisfaction as seen through the analysis of the all the four themes and their subsequent subthemes. Non-disclosure is complex issue in KSA which contrasts to the general perception of non-disclosure in the Western context. In the Western context, the patient is the key individual who is responsible for the decision making in terms of treatment, interaction with doctors and nurses, and acquires crucial information about their health which they deem sensitive. This Western form of non-disclosure links very closely to doctor-patient confidentiality. However, in the KSA setting non-disclosure is the total opposite as analysed from the findings. Non-disclosure in the KSA setting means that information regarding the health of the patient is disclosed to the family of the patient, and the family decides which information is disseminated to the patient.
The current study’s qualitative findings add to the plethora of knowledge of interpersonal aspects that was focused on healthcare professionals exclusively. However, the current study expands to the knowledge of how interpersonal aspects of care coupled with service organisation influenced the level of patient satisfaction in the KSA oncology ward settings. Through the evidence extracted from the findings it can be concluded that patient satisfaction is closely linked to specific contextual factors that are related to the themes which have been discussed in this chapter.
[1] Sitters are commonly relatives of the patients who, at the patients’ request accompany them during their hospitalisation, offering moral and practical support. Typically, patients are required to ask for their doctor’s permission to have a sitter stay with them overnight.
Conclusion
The current study was centred on the research question
What factors contribute to or hinder patient satisfaction with care in the oncology ward setting in the SRCC?
The aims that were used to answer the research question included determining how clinical effectiveness, accessibility to health care, and interpersonal aspects of care are associated with patient satisfaction in adult oncology settings in SRCC and how they may influence patient satisfaction. The current study has also aimed to provide recommendations to improve patient satisfaction in SRCC settings in Kingdom of Saudi Arabia oncology wards by conducting a mixed methods research which brought forth qualitative findings that strengthened quantitative results of patient satisfaction in the KSA setting,
It is clear from the findings that levels of patient satisfaction were based both on patients’ physical treatment and upon expectations as to the standard of care they hoped to receive. Not only was patients’ satisfaction with the quality of their care shaped by the nature, speed and efficiency of their treatment and the environment in which it takes place but it was also influenced by the sense that their psychological needs were being addressed as well as their physical health needs. Patients sought a caring and sensitive approach from their nurses and doctors and their satisfaction depended on strong interpersonal and individualised care. Patients also sought a patient-centred approach from both nurses and doctors.
Of particular importance is the fact that overall patients wished to be informed of their prognosis and treatments. This is contrary to the generally accepted traditional practice in the KSA, where physicians provide information about serious illnesses and treatments to family members first and seek approval before informing the patient. However, this norm is gradually being transitioned to become a -disclosure policy that conforms to the majority of patients’ opinions.
Doctors, nurses and healthcare organisations are seen by patients as providing not only physical care but also psychological support. This suggests the need for the development of strong doctor/nurse-patient relations and for healthcare providers in oncology ward settings to deliver a patient-centred approach. It is evident that the four emergent themes related to the patients’ needs to feel secure and have confidence in their nurses, doctors and health care setting. Therefore patients’ views must be taken into account if improvements in patient satisfaction and high-quality care are to be attained.
It would be pertinent to extend this research to a wider setting in a larger population to gain an even better understanding of the needs of patients, especially about their relationship with doctors and nurses in a multicultural setting. This examination of how to improve interpersonal relationships could then inform policymakers and ultimately lead to not only improved perceptions of the quality of their care but could also conceivably lead to real improvements in patient outcomes.
The current study has added valuable knowledge to the previously under-examined field of patient satisfaction with care in oncology ward settings in the KSA. It has highlighted factors that influence patients’ satisfaction with the quality of their care. In particular, it has provided evidence of a need for healthcare professionals in the oncology KSA health system to develop strong, interpersonal relations with their patients and practice a patient-centred approach. The new theories and fresh evidence provided by this research will be of substantial significance to policymakers and hospital management teams in the KSA wanting to improve the care of their patients in oncology wards.
References
Al-Borie, H.M. and Sheikh Damanhouri, A.M., 2013. Patients' satisfaction of service quality in Saudi hospitals: a SERVQUAL analysis. International journal of health care quality assurance, 26(1), pp.20-30.
Aboul-Enein, F. H. (2002). Personal contemporary observations of nursing care in Saudi Arabia. International Journal of Nursing Practice, 8(4), pp. 228-230.
Adib, S. M. (2004). From the biomedical model to the Islamic alternative: a brief overview of medical practices in the contemporary Arab world. Social Science and Medicine, 58(4), pp.697-702.
Aiken, L. H., Clarke, S. P., Sloane, D. M., Sochalski, J. A., Busse, R., Clarke, H., Giovannetti, P., Hunt, J., Rafferty, A. M. and Shamian, J. ( 2001). Nurses' reports on hospital care in five countries. Health Affairs, 20(3), pp. 43-53.
Akhtar, S. S. and Nadrah, H. M. (2005). Assessment of the quality of breast cancer care: A single institutional study from Saudi Arabia. International Journal for Quality in Health Care, 17(5). pp. 301-305.
Al-Ahmadi, H. and Roland, M. (2005). Quality of primary health care in Saudi Arabia: A comprehensive review. International Journal for Quality in Health Care, 17(4), pp. 331-346.
Al-Ahwal, M. (1998). Cancer patients’ awareness of their disease and prognosis. Ann Saudi Med, 18 (2) pp.187–189.
Alaloola, N. A. and Albedaiwi, W. A. (2008). Patient satisfaction in a Riyadh tertiary care centre. International Journal of Health Care Quality Assurance, 21(7), pp. 630-637.
Al-Amri, A. (2010). Saudi patients’ attitudes towards disclosure of cancer information. Middle East Journal of Cancer, 1(4), pp.175-180.
Al-Amri, A. and Sadat, A. (2009). Cancer chemotherapy-induced osteoporosis: How common is it among Saudi Arabian cancer survivors? Indian Journal of Cancer, 46(4), pp. 331-334.
Al-Ansary, L. and Alkhenizan, A. (2004).Towards evidence-based clinical practice guidelines in Saudi Arabia. Saudi Medical Journal, 25(11), pp.1555-1558.
Albrecht, G. L., Walker, V. G. and Levy, J. A. (1982). Social distance from the stigmatized: A test of two theories. Social Science and Medicine. 16, pp.1319–1327
Al-Dogaither, A. H. and Saeed, A. A. (2000). Consumers' satisfaction with primary health services in the city of Jeddah, Saudi Arabia. Saudi Medical Journal, 21(5), pp. 447-454.
Al-Doghaither, A. H. (2000). Inpatients’ satisfaction with nursing services at King Khalid University Hosptial, Riyadh, Saudi Arabia. Journal of Family Community Medicine, 7(3), pp. 37–45.
Al-Dossary, A., While, A. and Barriball, L. (2008). Health care and nursing in KSA. KSA International Nursing Review, 55(1), pp.125-128.
Al-Eid, H. S. and Manalo, M. S. (2007). Cancer Incidence and Survival Report. Saudi Arabia: Saudi Cancer Registry. [Online]. Available from: http://www.scr.org.sa/reports/SCR2007.pdf [Accessed 15 September 2011].
Al-Faris, E. A., Khoja, T., Falouda, M. and Saeed, A. (1996). Patients' satisfaction with accessibility and services offered in Riyadh health centres. Saudi Medical Journal, 17(1), pp. 11-17.
Aljubran, A. (2010). The attitude toward disclosure of bad news to cancer patients in Saudi Arabia. Annals of Saudi Medicine, 30(2), pp. 141-144.
Alkhenizan, A., & Shaw, C. (2011). Impact of accreditation on the quality of healthcare services: a systematic review of the literature. Annals of Saudi medicine, 31(4), 407.
AL-Malki, M., Fitzgerald, G. and Clark, M (2011). The nursing profession in KSAKSA: an overview. International nursing review, 58(3), pp. 304-311
Almoajel, Alyah M. (2012). Relationship between accreditation and quality indicators in hospital care: A review of the literature. World Applied Sciences Journal, 17(5), pp.598-606.
Al-Muzaini, A. S., Salek, M. S. and Nicholls, P.J. (1998). The attitude of health care professionals toward the availability of hospice services for cancer patients and their carers in Saudi Arabia. Palliative Medicine, 12(5), pp. 365–373.
Al-Rubaiee, L. (2011).The mediating effect of patient satisfaction in the patients' perceptions of healthcare quality: Patient trust relationship. International Journal of Marketing Studies, 3(1), p.103.
AL-Sakkak, M.A., AL-Nowaiser, N.A., AL-Khashan, H.I., AL-ABdrabulnabI, A.A. and JABER, R.M., (2008) Patient satisfaction with primary health care services in Riyadh. Saudi Medical Journal, 29(1), pp. 432-436.
Al-Shahri, M. (2002).Culturally sensitive caring for Saudi patients. Journal of Transcultural Nursing, 13(2), pp.133-138.
Al-Sirafy, S. A., Hassan, A. A. and al-Shahri, M. Z. (2009). Hospitalization pattern in a hospital-based palliative care program: An example from Saudi Arabia. American Journal of Hospice and Palliative Medicine, 26(1), pp. 52-56.
Altschul, A. (1971). Relationships between patients and nurses in psychiatric wards. International Journal of Nursing Studies, 8 (3), pp.179–187.
Al-Zayyer, W. (2003). The effectiveness of recruitment and retention strategies and the severity of recruitment and retention barriers of staff nurses in selected tertiary care hospitals in KSA. PhD thesis, George Mason University.
Andersen, M. R., Bowen, D. J., Morea, J., Stein, K. D. and Baker, F. (2009). Involvement in decision-making and breast cancer survivor quality of life. Health Psychology, 28(1), pp.29-37.
Anhang Price, R., Elliott, M.N., Zaslavsky, A.M., Hays, R.D., Lehrman, W.G., Rybowski, L., Edgman-Levitan, S. & Cleary, P.D. (2014), "Examining the Role of Patient Experience Surveys in Measuring Health Care Quality", Medical Care Research and Review, 71( 5), pp. 522-554.
Ansmann, L., Kowalski, C., Ernstmann, N., Ommen, O., Jung, J., Visser, A. and Pfaff, H. (2013). Do breast cancer patients receive less support from physicians in German hospitals with high physician workloads? A multilevel analysis. Patient education and counselling, 93(2), pp.327-334.
Ansmann, L., Kowalski, C., Ernstmann, N., Ommen, O., Jung, J., Visser, A. and Pfaff, H. (2013). Do breast cancer patients receive less support from physicians in German hospitals with high physician workloads? A multilevel analysis. Patient Education and Counselling, 93(2), pp. 327-334.
Arai, L., Britten, N., Popay, J., Roberts, H., Petticrew, M., Rodgers, M. and Sowden, A. J. (2007). Testing methodological developments in the conduct of narrative synthesis: A demonstration review of research on the implementation of smoke alarm interventions. Evidence and Policy: A Journal of Research, Debate and Practice, 3(3), pp.361-383.
Armstrong, R., Jackson, N., Doyle, J., Waters, E. and Howes, F. (2005). It’s in your hand: The value of hand searching in conducting systematic reviews of public health interventions. Journal of Public Health, 27(4), pp. 388-391.
Arora ,N.(2003). Interacting with cancer patients: Significance of physicians’ communication behaviour. Social Science and Medicine, 57 (5), pp. 791-806.
Arora, V., Philp, S., Nattress, K., Pather, S., Dalrymple, C., Atkinson, K., ... and Carter, J. (2010). Patient satisfaction with inpatient care provided by the Sydney Gynecological Oncology Group. Patient-related outcome measures, 1, 179-184.
Arraras J. I., Vera, R., Martínez, M., Hernández, B., Laínez, N., Rico, M., Vila, M., Chicata, V. and Asín, G. (2009). The EORTC cancer in-patient satisfaction with care questionnaire: EORTC IN-PATSAT32 validation study for Spanish patients. Clinical and Translational Oncology, 11(4), pp. 237-42.
Arthur, S. and Nazroo, J. (2003). Designing fieldwork strategies and materials. In: Ritchie, J. and Lewis, J., eds, Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage, pp. 109-137.
Atallah, M., Hamdan-Mansour, A., al-Sayed, M. and Aboshaiqah, A. (2013). Patients' satisfaction with the quality of nursing care provided: The Saudi experience. International Journal of Nursing Practice, 19(6), pp. 584–590.
Barbour, R. S. (1999). The case for combining qualitative and quantitative approaches in health services research. Journal of Health Services Research and Policy. 4, pp. 39-43.
Barlesi, F., Boyer, L., Doddoli, C., Antoniotti, S., Thomas, P., and Auquier, P. (2005). The place of patient satisfaction in quality assessment of lung cancer thoracic surgery. Chest Journal, 128(5), pp.3475-3481.
Barriball K.L., Christian S.L., While A.E. and Bergen A. (1996). The telephone survey method: a discussion paper. Journal of Advanced Nursing, 24 (1) pp.115 – 121.
Barriball, K. and While, A. (1994). Collecting data using a semi‐structured interview: A discussion paper. Journal of Advanced Nursing. 19(2), pp. 328-335.
Batbaatar, E., Dorjdagva, J., Luvsannyam, A., & Amenta, P. (2015). Conceptualisation of patient satisfaction: a systematic narrative literature review. Perspectives in public health,
Bazeley, P. and Jackson, K., eds. (2013). Qualitative data analysis with NVivo. Sage Publications Limited.
Beattie, M., Lauder, W., Atherton, I., & Murphy, D. J. (2015). Instruments to measure patient experience of health care quality in hospitals: a systematic review. Syst Rev, 3, 4.
Bleich, S. N., Özaltin, E., & Murray, C. J. (2009). How does satisfaction with the healthcare system relate to patient experience? Bulletin of the World Health Organization, 87(4), 271-278.
Beaver, K., Luker, K., Owens, R., Leinster, S., Degner, L. and Sloan, J. A. (1996). Treatment decision making in women newly diagnosed with breast cancer. Cancer Nursing. 19(1), pp. 8-19.
Bedikian, A. Y., Saleh, V. and Ibrahim, S. (1985). Saudi patient and companion attitudes toward cancer. The King Faisal Specialist Hospital Medical Journal. 5(17), pp. 25-29.
Beebe, J (2001). Rapid Assessment Process: An Introduction. Oxford: Alta Mira Press:
Beling, W. A. (1980). King Faisal and the Modernisation of Saudi Arabia. King Faisal and the Modernisation of Saudi Arabia.
Bertakis, K., Roter, D. and Putnam, S. (1999). The relationship of physician medical interview style to patient satisfaction. Journal of Family Practice, 32 (2), pp.175-181.
Bialor, B. D., Musial, J. L., Rojas, G. E. and Fagan, M. J. (1999). Use of an open-ended question to supplement a patient satisfaction questionnaire in a medical residents' clinic. American Journal of Managed Care. 5(12), pp. 1542-1549.
Bilimoria, K. Y., Bentrem, D.J., Stewart, A. K., Winchester, D. P. and Ko, C. Y. (2009). Comparison of commission on cancer-approved and –non-approved hospitals in the United States: Implications for studies that use the National Cancer Data Base. Journal of Clinical Oncology, 27(25), pp. 4177-81.
Blanchard, C. G., Labrecque, M. S., Ruckdeschel, J. C. and Blanchard, E. B. (1990). Physician behaviours, patient perceptions, and patient characteristics as predictors of satisfaction of hospitalized adult cancer patients. Cance,. 65, pp. 186-192.
Bleich SN, Özaltin E, Murray CJ (2009) How does satisfaction with the healthcare system relate to patient experience? Bull World Health Organ 87(4) pp.271–278
Borras, J. M., Sanchez-Hernandez, A., Navarro, M., Martinez, M., Mendez, E., Ponton, J. L. L., ... and Germa, J. R. (2001). Compliance, satisfaction, and quality of life of patients with colorectal cancer receiving home chemotherapy or outpatient treatment: a randomised controlled trial. BMJ, 322 (7290), pp.826-830
Bourdon, S. (2002). The integration of qualitative data analysis software in research strategies: Resistances and possibilities. Forum: Qualitative Social Research. 3(2), Art.11.
Bowling, A. (2002). Speaker's Corner: An “inverse satisfaction law”? Why don't older patients criticise health services? Journal of Epidemiology and Community Health. 56(7), p. 482.
Bowling, A. (2007). Research Methods in Health: Investigating Health and Health Services. 2nd ed. Open University Press; Maidenhead, U.K.
Bowling, A., Rowe, G. And McKee, M. (2013). Patients' experiences of their healthcare about their expectations and satisfaction: A population survey. Journal of the Royal Society of Medicine, 106(4), pp.143-9.
Bowman, G. S., Howden, J., Allen, S., Webster, R. A., and Thompson, D. R. (1994). A telephone survey of medical patients 1 week after discharge from hospital. Journal of Clinical Nursing, 3(6), 369-373.
Boyatiz, R. (1998). Transforming Qualitative Information: Thematic Analysis and Code Development. Thousand Oaks, CA: Sage.
Boyles, C. and Nordhaugen, N. (1989). An employee health service in Saudi Arabia. American Association of Occupational Health Nurses Journal, 37(11), pp. 459–64.
Brady, M. K., and Cronin, J. J. Jr. (2001). Some new thoughts on conceptualizing perceived service quality: A hierarchical approach. Journal of Marketing, 65(July), pp. 34-49.
Bredart, A. Coens, C. Aaronson, N., Chie, W. C., Efficace, F. Conroy, T., Blazeby, J. M., Hammerlid, E., Costantini, M., Joly, F., Schraub, S., Sezerl, O., Arraras, J. I., Rodary, C., Costantini, A., Mehlitz, M., Razavi, D. and Bottomley, A. (2007). Determinants of patient satisfaction in oncology settings from European and Asian countries: Preliminary results based on the EORTC IN-PATSAT32 questionnaire. European Journal of Cancer, 43(2), pp. 323-330.
Bredart, A., Bottomley, A., Blazeby, J. M., Conroy, T., Coens, C., D’haese, S., Chie, W., Hammrelid, E., Arraras, J. I., Efficace, F., Rodary, C., Schraub, S., Costantini, M., Costantini, A., Joly, F., Sezer, O., Razavi, D., Mehlitz, M., Bielska-Lasota, M. and Aaronson, N. K. (2005). An international prospective study of the EORTC cancer in-patient satisfaction with care measure (EORTC IN-PATSAT32). European Journal of Cancer, 41(14), pp. 2120-2131.
Brédart, A., Razavi, D., Delvaux, N., Goodman, V., Farvacques, C. and Van Heer, C.(1998). A comprehensive assessment of satisfaction with care for cancer patients. Supportive Care in Cancer, 6(6), pp. 518-523.
Bredart, A., Razavi, D., Robertson, C., Didier, F., Scaffidi, E. and de Haes, J. (1999). A comprehensive assessment of satisfaction with care: Preliminary psychometric analysis in an oncology institute in Italy. Annals of Oncology, 10(7), pp. 839-846.
Brédart, A., Robertson, C., Razavi, D., Batel-Copel, L., Larsson, G., Lichosik, D., Meyza, J., Schraub, S., von Essen, L. and de Haes, J. (2003). Patients' satisfaction ratings and their desire for care improvement across oncology settings from France, Italy, Poland and Sweden. Psycho-Oncology, 12(1), pp. 68–77.
Brett, A. S. and McCullough, L. B. (2012). Addressing requests by patients for non-beneficial interventions. Journal of the American Medical Association, 307(2), pp.149-150.
Brislin, R. W., Lonner, W. and Thorndike, R. M. (1973). Cross-Cultural Research Methods. New York: John Wiley and Sons.
Brown, S., Belgaumi, A., Kofide, A., Sabbah, R., Ezzat, A., Littlechild, B., Shoukri, M., Barr, R. and Levin, A. (2009). Failure to attend appointments and loss to follow-up: A prospective study of patients with malignant lymphoma in Riyadh, Saudi Arabia. European Journal of Cancer Care,18(3), pp. 313-317.
Bryman, A. (2004). Social Research Methods. 2nd ed. New York: Oxford University Press.
Bryman, A. (2006). Integrating quantitative and qualitative research: How is it done? Qualitative Research, 6(1), pp. 97–113.
Burnett, J. R., Fan, C., Motowidlo, S. J., and Degroot, T. (1998). Interview notes and validity. Personnel Psychology, 51(2), 375-396.
Burns, N. and Grove, S. (2007). Understanding Nursing Research: Building an Evidence-Based Practice. 4th ed. Elsevier Saunders: Edinburgh.
Calman, L. (2006). Patients’ views of nurses’ competence. Nurse Education Today, 26(8) pp. 719-725.
Campbel,l J. L., Ramsay, J. and Green, J. (2001). Age, gender, socioeconomic, and ethnic differences in patients’ assessments of primary health care. Quality in Health Care. 10(2), pp. 90–95.
Campbell, S., Roland, M. and Buetow, S. (2000). Defining quality of care. Social Science and Medicine, 51(11), pp. 1611-1625.
Carr-Hill, R. A. (1992). The measurement of patient satisfaction. Journal of Public Health, 14(3), 236-249.
Carmel, S. and Glick, S. M. (1996). Compassionate-empathic physicians: Personality traits and social-organizational factors that enhance or inhibit this behaviour pattern. Social Science and Medicine, 43(8), pp. 1253-1261.
Cecil, D. W. and Killeen, I., (1997). Control, compliance, and satisfaction in the family practice encounter. Family Medicine. 29(9), pp. 653-657.
Central Department of Statistics and Information (2010), Kingdom of Saudi Arabia, Estimate of population by sex and nationality in the kingdom for the years (2004-2014) [Accessed online from] http://www.cdsi.gov.sa/english/index.php?option=com_docman&Itemid=160
Chapple, A., Ziebland, S. and McPherson, A. (2004). Stigma, shame, and blame experienced by patients with lung cancer: Qualitative study. BMJ, 328(7454), pp. 1470-1473.
Chassin, M. R., Gavin, R. W. (1998). The urgent need to improve health care quality: Institute of Medicine National Round Table on Health Care Quality. Journal of the American Medical Association, 280(11), pp. 1000–1005.
Cleary, P. D. (1998). Satisfaction may not suffice! International Journal of Technology for Assessing Health Care. 14(1), pp. 35–37.
Cleary, P. D. and Edjman-Levitan, S. (1997). Health care quality: Incorporating consumer perspectives. Journal of the American Medical Association,278(19), pp. 1608-1612.
Cleary, P. D., Keroy, L., Karapanos, G. and McMullen, W. (1989). Patient assessment of hospital care. Quality Review Bulletin.15(6), pp.172-179.
Clever, S., Jin, L., Levinson, W. and Meltzer, D. (2008). Does doctor-patient communication affect patient satisfaction with hospital care? Results of an analysis with a novel instrumental variable. Health Services Research. 43(5p1), pp. 1505-1519.
Cohen (1996). Age and health status in a patient satisfaction survey. Social Science and Medicine, 42 (7), pp.1085-1093
Cohen, L., Manion, L. and Morrison, K. (2007). Research Methods in Education. 6th ed. Routledge: London.
Collins, K. M. T., Onwuegbuzie, A. J. and Sutton, I. L. (2006). A model incorporating the rationale and purpose for conducting mixed-methods research in special education and beyond. Learning Disabilities: A Contemporary Journal. 4(1), pp.67-100.
Cornell, B., Hagger, V., Wilson, S. G., Evans, S. M., Sprivulis, P. C. and Cameron, P. A. (2009). Measuring the quality of hospital care: An inventory of indicators. Internal Medicine Journal, 39(6), pp. 352-360.
Coughlan, M., Cronin, P. and Ryan, F. (2013). Doing a Literature Review in Nursing, Health and Social Care. London: Sage.
Coyle, J. and Williams, B. (2000). An exploration of the epistemological intricacies of using qualitative data to develop a quantitative measure of user views of health care. Journal of Advanced Nursing. 31(5), pp. 1235–1243.
Crabtree, B. and Miller, W. (1999). A template approach to text analysis: Developing and using codebooks. In: Crabtree, B. and W. Miller, eds. Doing Qualitative Research. Newbury Park, CA: Sage, pp. 163-177.
Creswell, J. and Plano Clark, V. (2007). Designing and Conducting Mixed Methods Research. Thousand Oaks, CA: Sage Publications.
Creswell, J. and Tashakkori, A. (2007). Differing perspectives on mixed methods research. Journal of Mixed Methods Research. 1(4), pp. 303-308.
Creswell, J. W. (1998). Qualitative Inquiry and Research Design: Choosing Among Five Traditions. Thousand Oaks: Sage Publications.
Creswell, J. W. (2009). Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. 3rd ed. Thousand Oaks, CA: Sage Publications.
Creswell, J. W., V. L. Plano Clark, M. Gutmann, and W. Hanson. (2003). Advanced mixed methods research designs. In Handbook on mixed methods in the behavioural and social sciences, ed. A. Tashakkori and C. Teddlie, 209-240. Thousand Oaks, CA: Sage.
Cronholm, S. and Hjalmarsson, A. (2011). Experiences from sequential use of mixed methods. The Electronic Journal of Business Research Methods. 9(2), pp. 87-95.
Crow, R., Gage, H., Hampson, S., Hart, J., Kimber, A., Storey, L., Thomas, H. (2002). The measurement of satisfaction with healthcare: Implications for practice from a systematic review of the literature. Health Technology Assessment, 6(32), pp.1–244.
Cull, A., Sprangers, M. and Bjordal, K. (2002). Guidelines for translating EORTC Questionnaires. Quality of Life Study Group Publications. Brussels: EORTC Publication.
Cull, A., Stewart, M., & Altman, D. G. (1995). Assessment of and intervention for psychosocial problems in routine oncology practice. British Journal of Cancer, 72(1), pp. 229.
Daly, J., Kellehear, A. and Gliksman, M. (1997). The Public Health Researcher: A Methodological Approach. Melbourne, Australia: Oxford University Press.
Data Protection Act (1998), Data Protection Act.
Datta, L. (1997). Multimethod evaluations: Using case studies together with other methods. In: Chelimsky, E. and Shadish. W. R., eds. Evaluation for the 21st Century: A Handbook. Thousand Oaks, CA: Sage Publications, pp. 344–359.
Davies, H. and Crombie, I (1995). Assessing the quality of care. BMJ, 311(7008), p. 766.
De Silva, D. (2014). Helping measure person-centred care: A review of evidence about commonly used approaches and tools used to help measure person-centred care. London: The Health Foundation.
Dein, S. and Stygall, J. (1997).Does being religious help or hinder coping with chronic illness? A critical literature review. Palliative Medicine,11(4), pp. 291–298.
Diab, R. (2010). Access to Cancer Care Facilities: Initiative to Improve Cancer Care in the Arab World. Riyadh: National Guard Health Affairs.
Dieronitou, I. (2014).The ontological and epistemological foundations of qualitative and quantitative approaches to research. International Journal of Economics, Commerce and Management, 2 (10), pp.1-17.
Dixon-Woods, M., Kirk, D., Agarwal, S., Annandale, E., Arthur, T., Harvey, J., Hsu, R., Katbamna, S., Olsen, R., Smith, L., Riley, R. and Sutton, A. (2005). Vulnerable Groups and Access to Health Care: A Critical Interpretive Review. London: National Coordinating Centre for the Service Delivery and Organisation (NCCSDO) Research Programme.
Doering, E. (1983). Factors influencing inpatient satisfaction with care. Quality Review Bulletin, 9, pp. 291-299.
Donabedian (1988). The quality of care. How can it be assessed? JAMA, 260 (12),pp.1743-1748
Donabedian, (1980). Explorations in quality assessment and monitoring. Vol. 1. The definition of quality and approaches to its assessment. Ann Arbor, Mich.: Health Administration Press
Dowling, M. (2008). The meaning of nurse–patient intimacy in oncology care settings: From the nurse and patient perspective. European Journal of Oncology Nursing. 12(4), pp. 319-328.
Draper, M., Cohen, P., and Buchan, H. (2001). Seeking consumer views: what use are results of hospital patient satisfaction surveys? International Journal for Quality in Health Care, 13(6), 463-468.
Duff, B. (2013). Creating a culture of safety by coaching clinicians to competence. Nurse Education Today, 33(10), pp. 1108-1111.
Duffield, C., Diers, D., O’Brien-Pallas, L., Aisbett, C., Roche, M., King, M. and Aisbett, K.( 2011). Nursing staffing, nursing workload, the work environment and patient outcomes. Applied Nursing Research, 24(4), pp. 244-255.
DuFrene R., (2000). An evaluation of a patient satisfaction survey: Validity and reliability. Evaluation and Program Planning. 23(3), pp 293-300.
Eaves, S., and Walton, J. (2013). Mixed Methods Research: Creating Fusion from the QUAL and QUAN Data Mosaic. In Proceedings of The 12th European Conference on Research Methodology for Business and Management Studies. Reading, UK, Academic Conferences and Publishing International Limited (pp. 118-126).
El Saghir, N. and Azim, H. (2010). Standards of Care and Guidelines for the Arab World with Limited Resources: Initiative to Improve Cancer Care in the Arab World. Riyadh: National Guard Health Affairs.
Elkum, N., Dermime, S., Ajarim, D., al-Zahari, A., Alsayed, A., Tulbah, A., al-Amalik, O., Alshabanah, M., Ezzat, A. and al-Tweigeri, T. (2007) Being 40 or younger is an independent risk factor for relapse inoperable breast cancer patients: The Saudi Arabia experience. BMC Cancer. 7 (1) 222. Available from: <http://www.biomedcentral.com/1471-2407/7/222>.
Elzubier, A. ( 2002). Doctor-patient communication: A skill needed in KSA. Saudi Journal of Family and Community Medicine. 9(1), pp. 51-56.
Epstein, R. and Street, J (2007) Patient-centred communication in cancer care: promoting healing and reducing suffering. Bethesda, MD: National Cancer Institute, NIH Publication No.07-6225.
Epstein, R. and Street, J. (2007). Patient-centred communication in cancer care: Promoting healing and reducing suffering. Bethesda, MD: National Cancer Institute (NIH Publication No.07-6225).
Erlandson, D., Harris, E., Skipper, B. and Allen, S. (1993). Doing Naturalistic Inquiry: A Guide to Methods. Thousand Oaks, CA: Sage Publication.
Ervin, N. E. (2006). Does patient satisfaction contribute to nursing care quality? Journal of Nursing Administration, 36(3), pp. 126–130.
Ezzat, A., Gray, A. J. and Volker, S. (1995). Developing palliative care services for terminally ill patients in Saudi Arabia. Annals of Saudi Medicine, 15(4), pp.370– 377.
Fallowfield, L., Ratcliffe, D., Jenkins, V., & Saul, J. (2001). Psychiatric morbidity and its recognition by doctors in patients with cancer. British Journal of Cancer, 84(8), pp. 1011.
Feilzer, M. (2010). Doing mixed methods research pragmatically: Implications for the rediscovery of pragmatism as a research paradigm. Journal of Mixed Methods Research, 4(1), pp. 6-16.
Fereday, J. and Muir-Cochrane, E. ( 2006). Demonstrating rigour using thematic analysis: A hybrid approach of inductive and deductive coding and theme development. International Journal of Qualitative Methods, 5(1) pp.1-11.
Field, D. and Copp, G. (1999). Communication and awareness about dying in the 1990s. Palliative Medicine. 13 (6) pp.459 -468
Findik, U. Y., Unsar, S. and Sut, N. ( 2010). Patient satisfaction with nursing care and its relationship with patient characteristics. Nursing and Health Sciences, 12(2), pp. 162-169.
Fogarty, L. A., Curbow, B. A., Wingard, J. R., Mcdonnell, K. and Somerfield, M. R. (1999). Can 40 Seconds of Compassion Reduce Patient Anxiety? Journal of Clinical Oncology, 17(1), pp. 371-379.
Fontana, A. and Frey, J. (1994). Interviewing: The art of science. In Denzin, N. and Lincoln, Y. Handbook of Qualitative Research. London: Sage Publications.
Gaston, C. M., and Mitchell, G. (2005). Information giving and decision-making in patients with advanced cancer: a systematic review. Social science and medicine, 61(10), pp.2252-2264.
Gill, L. and White, L. (2009). A critical review of patient satisfaction. Leadership in Health Services, 22(1) pp. 8-19.
Given, B. A., Given, C. W. and Kozachik, S.( 2001). Family support in advanced cancer. A Cancer Journal for Clinicians. 51(4), pp. 213-231.
Goffman, E. (1963). Stigma: Notes on the Management of Spoiled Identity. Harmondsworth: Penguin Books.
Gordon R.L. (1975) Interviewing: Strategy, Techniques and Tactics. Dorsey Press, Illinois.
Gotlieb, J. B. (2000). Understanding the effects of nurses, patients' hospital rooms, and patients' perception of control on the perceived quality of a hospital. Health Marketing Quarterly. 18(1-2), pp. 1-14.
Green, J. and Thorogood, N. (2009). Qualitative Methods for Health Research. 2nd ed. London: Sage.
Greene, J. C. (2007). Mixed methods in social inquiry (Vol. 9). John Wiley & Sons.
Greene, J. C., Caracelli, V. J. and Graham, W. F. (1989). Toward a conceptual framework for mixed-method evaluation designs. Education Evaluation and Policy Analysis, 11(3), pp. 255–274.
Griffin, S.J., Kinmonth, A.L., Veltman, M.W., Gillard, S., Grant, J. and Stewart, M. (2004). Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Annals of Family Medicine, 2 (6) pp.595-608.
Griffiths, P., Simon, M., Richardson, A. & Corner, J. 2013, "Is a larger specialist nurse workforce in cancer care associated with better patient experience? Cross-sectional study", Journal of health services research & policy, vol. 18, no. 1, pp. 39-46.
Groene, O., Skau J. K. and Frolich, A. (2008). An international review of projects on hospital performance assessment. International Journal of Quality Health Care. 20(3), pp.162–71.
Gronroos, C. (2000). Service Management and Marketing: A Customer Relationship Management Approach. New York, NY: Wiley.
Guba, E. G. (1990). The alternative paradigm dialogue. In Guba, E. G., ed. The Paradigm Dialog. Newbury Park, CA: Sage, pp. 17-27.
Guba, E. G. and Lincoln, Y. S. (1994). Competing paradigms in qualitative research. In Denzin N. K. and Y. S.Lincoln, eds. Handbook of Qualitative Research. Thousand Oaks, CA: Sage.
Haberfelde, M., Bedecarré, D. and Buffum, M. (2005). Nurse-sensitive patient outcomes: An annotated bibliography. Journal of Nursing Administration, 35(6), pp. 293-299.
Haddad, S., Potvin, L., Roberge, D., Pineault, R. and Remondin, M. (2000). Patient perception of quality following a visit to a doctor in a primary care unit. Family Practice, 17(1), pp. 21–29.
Hall, J. A. and Dornan, M. C. (1990). Patient socio-demographic characteristics as predictors of satisfaction with medical care: A meta-analysis. Social Science and Medicine,30, pp. 811-818.
Halldorsdottir, S. and Hamrin, E. (1997). Caring and uncaring encounters within nursing and health care from the cancer patient's perspective. Cancer nursing, 20(2) pp.120-128.
Hallenbeck, J., and Arnold, R. (2007). A request for nondisclosure: Don't tell the mother. Journal of Clinical Oncology, 25(31), pp. 5030-5034.
Halligan, P. (2006). Caring for patients of Islamic denomination: critical care nurses’ experiences in Saudi Arabia. Journal of Clinical Nursing, 15(12), pp.1565-1573.
Hamer, M., Chida, Y., and Molloy, G. J. (2009). Psychological distress and cancer mortality. Journal of psychosomatic research, 66(3), pp.255-258.
Hammersley, M. (1996). The relationship between qualitative and quantitative research: Paradigm loyalty versus methodological eclecticism. In Richardson, J. T. E., ed. Handbook of Qualitative Research Methods for Psychology and Social Sciences. Wiley-Blackwell. pp. 159-174.
Hanson, W. E., Creswell, J. W., Plano Clark, V., Petska, K. S. and Creswell, J. D. (2005). Mixed method design in counselling psychology. Journal of Counselling Psychology. 52(2), pp.224–235.
Harris L. R., and Brown, G.T.L. (2010). Mixing interview and questionnaire methods: Practical problems in aligning data. Practical Assessment, Research and Evaluation. 15(1), pp. 1-19. Available online: <http://pareonline.net/pdf/v15n1.pdf>.
Harwell M R (2013). Research Design in Qualitative/Quantitative/Mixed Methods In Pursuing Ideas as the Keystone of Exemplary Inquiry, Second Edition Clifton F. Conrad and Ronald C. London: Sage, p147-182
Haskard Zolnierek, K. and DiMatteo, M. (2009). Physicians communication and patient adherence to treatment: A meta-analysis. Medical Care. 47(8), pp. 826-834.
Health Foundation (2013) Measuring patient experience, No 18 Evidence Scan. [Accessed online] on 12 August 2015 from http://www.health.org.uk/sites/default/files/MeasuringPatientExperience.pdf
Heath, I., Rubinstein, A., Stange, K. C., and van Driel, M. L. (2009). Quality in primary health care: a multidimensional approach to complexity. BMJ, 338 (b1242)
Hennekens, C. H., Buring, J. E. (1987). Epidemiology in Medicine. Lippincott Williams and Wilkins.
Hobbs, J. L. (2009). A dimensional analysis of patient-centered care. Nursing Research. 58(1), pp. 52-62.
Holmstrom, I. and Roing, M. (2010). The relation between patient-centeredness and patient empowerment: A discussion on concepts. Patient Education and Counselling, 79(2), pp.167-172.
Hopton, J. L., Howie, J. G. R. and Porter, M. D. (1993). The need for another look at the patient in General Practice satisfaction surveys. Journal of Family Practice. 10(1), pp.82-87.
Hutchinson, C. L., Roffers, S. D., Fritz, A. D., eds. (2004). Cancer Registry Management: Principles and Practice. 2nd ed. Alexandria, VA: National Cancer Registrar’s Association.
Hyrkäs, K. and Paunonen, M. (2000). Patient satisfaction and research-related problems (part 2). Is triangulation the answer? Journal of Nursing Management. 8(4), pp. 237–245.
Ibrahim, E., Al Saad, R., Wishi, A., Khafaga, Y., el Hussainy, G. and al-Amro, A. (2002). Appraisal of communication skills and patients’ satisfaction in cross-language encounters in oncology practice. Journal of Cancer Education.17(4), pp.216-221.
Ibrahim, E., Sadiq, B. M. B., Banjar, L., Awadalla, S., & Abomelha, M. S. (2008). Current and future cancer burden in Saudi Arabia: meeting the challenge. Haematology/oncology and stem cell therapy, 1(4), 210-215.
Ibrahim, I., ZeenEldin, A., Bin Sadiq, B. and Ezzat, A. (2008). The present and the future of breast cancer burden in the Kingdom of Saudi Arabia. Journal of Medical Oncology. 36(155), pp.387-393.
Initiative to Improve Cancer Care in the Arab World (ICCAW) (2010). Proceedings of the Symposium. Riyadh: National Guard Health Affairs. Available online from: <http://amaac.org/images/PAJO_march_2010.pdf>. [Accessed on 12-01-2012].
Institute of Medicine (IOM) (2001). Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press. Available online from: http://www.iom.edu/Reports/2001/Crossing-the-Quality-Chasm-A-New-Health-System-for-the-21st-Century.aspx [Accessed on 25 Aug 2012].
International Alliance of Patients’ Organisations, IAPO (2009). Declaration of Patient-Centred Healthcare, London, UK.
International Council for Nurses ICN (2005). Competencies framework for the Nurse Specialist. ICN regulation series, Geneva: Switzerland
Irvine, A., Drew, P. and Sainsbury, R. (2013). Am I not answering your questions properly? Clarification, adequacy and responsiveness in semi-structured telephone and face-to-face interviews. Qualitative Research, 13(1), pp. 87-106.
Irvine, D., and Donaldson, L. (1993). Quality and standards in health care. Proceedings of the Royal Society of Edinburgh, Section B. Biological Sciences, 101, 1-30
Jackson J. L., Chamberlin J. and Kroenke, K. (2001). Predictors of patient satisfaction. Social Science and Medicine, 52(4), pp. 609-620.
Jacobs, R., Mannion, R., Davies, H.T.O., Harrison, S., Konteh, F. and Walshe, K. (2013). The relationship between organizational culture and performance in acute hospitals. Social Science and Medicine, 76 (1), pp.115-125.
Jagosh, J., Boudreau, J. D., Steinert, Y., MacDonald, M. E. and Ingram. L. (2011). The importance of physician listening from the patients’ perspective: Enhancing diagnosis, healing, and the doctor–patient relationship. Patient Education and Counselling, 85(3), pp. 369–374.
Jaipaul, C. K. and Rosenthal, G. E. (2003). Are older patients more satisfied with hospital care than younger patients? Journal of General Internal Medicine, 18(1), pp. 23–30.
Janesick, V. (2003). The choreography of qualitative research: Minuets, improvisations, and crystallization. In: Denzin, N. and Lincoln, Y. S., eds. Strategies of Qualitative Inquiry. Thousand Oaks, CA: Sage Publications, pp. 46–79.
Jazieh, A. R. (2010). Human Resources Development: Initiative to Improve Cancer Care in the Arab World. Riyadh: National Guard Health Affairs.
Jazieh, A., Al-Khatib, S. and Abulkhair, O. (2010). Initiative to Improve Cancer Care in the Arab World Inaugural Meeting Report. Available online from: <http://2010.iccaw.com/objects/PAORGInagauralMeeting.pdf>.
Jazieh, Abdul Rahman (2012). Cancer Care in Saudi Arabia: An interview with International Affairs Committee member Abdul-Rahman Jazieh. Available online from < http://connection.asco.org/magazine/article/id/3141/cancer-care-in-saudi-arabia.aspx>.
Johansson, P., Oléni, M. and Fridlund, B. (2002). Patient satisfaction with nursing care in the context of health care: A literature study. Scandinavian Journal of Caring Sciences. 16(4), pp. 337-344.
Johnson, R. B., Onwuegbuzie, A. J. and Turner, L. A. (2007). Toward a definition of mixed methods research. Journal of Mixed Methods Research. 1(2), pp.112-133.
Kaba, R. and Sooriakumaran, P. (2007). The evolution of the doctor-patient relationship. International Journal of Surgery. 5(1), pp. 57-65.
Kaiser, H. F. (1974). An index of factorial simplicity. Psychometrika, 39(1), pp.31-36.
Keith, R. (1998). Patient satisfaction and rehabilitation services. Archives of Physical Medicine and Rehabilitation,79(9) pp.1122-8.
Kenny, D. A., Veldhuijzen, W., Weijden, T., LeBlanc, A. and Lockyer, J. et al. (2010). Interpersonal perception in the context of doctor–patient relationships: A dyadic analysis of doctor–patient communication. Social Science and Medicine. 70(5), pp. 763-768.
Khamis, K., and Njau, B. (2014).Patients' level of satisfaction with the quality of health care at Mwananyamala Hospital in Dar es Salaam, Tanzania. BMC health services research, 14(1), pp. 400-407
Khayat, K. and Salter, B. (1994). Patient satisfaction surveys as a market research tool for general practices. British Journal of General Practice. 44(382), pp. 215-219.
Khbari, F., Hosseini, M., Arab, M. and Chozokly, N. (2006). Study of effective factors on inpatient satisfaction in hospitals of Tehran University of Medical Science. Scientific Journal of School of Public Health and Institute of Public Health Research. 4(3), pp. 25-36.
King, M., Jones, L. and Richardson, R. (2008). The relationship between patients’ experiences of continuity of cancer care and health outcomes: A mixed methods study. British Journal of Cancer. 98(3), pp. 529-536.
King, N., and Horrocks, C (2010). Interviews in Qualitative Research. London; Sage.
Kleeberg, U. R., Tews, J. T., Ruprecht, T., Höing, M., Kuhlmann, A., and Runge, C. (2005). Patient satisfaction and quality of life in cancer outpatients: results of the PASQOC* study. Supportive care in cancer, 13(5), pp.303-310.
Kringos, D. S., Boerma, W. G., Bourgueil, Y., Cartier, T., Hasvold, T., Hutchinson, A., and Wilm, S. (2010). The European primary care monitor: structure, process and outcome indicators. BMC family practice, 11 (1), 81
Krupat, E., Bell, R. A., Kravitz, R. L., Thom, D., and Azari, R. (2001). When physicians and patients think alike: patient-centred beliefs and their impact on satisfaction and trust. Journal of Family Practice, 50(12)pp. 1057-1062.
Kupfer, J. and Bond, E. (2012). Patient satisfaction and patient-centred care: Necessary but not equal. Journal of the American Medical Association, 302(2), pp.139-140.
Ladhari, R. (2009). A review of twenty years of SERVQUAL research. International Journal of Quality and Service Sciences, 1(2), 172-98.
Lankshear, A. J., Sheldon, T. A. and Maynard, A. ( 2005). Nurse staffing and healthcare outcomes: A systematic review of the international research evidence. Advances in Nursing Science, 28(2), pp. 163-174.
Lincoln Y.S. and Guba E.G. (2000) Paradigmatic controversies, contradictions, and emerging confluences. In Handbook of Qualitative Research, Vol. 2 (eds N.K. Denzin and Y.S. Lincoln), pp. 163–188. Sage Publications, Thousand Oaks, CA.
Lincoln, Y. S. and Guba, E. (1985). Naturalistic Inquiry. Thousand Oaks, CA: Sage.
Linder-Pelz, S. (1982). Toward a theory of patient satisfaction. Social Science and Medicine,16(5), pp. 577-82.
Little, P., Everitt, H., Williamson, I., Warner, G., Moore, M., Gould, C., Ferrier, K. and Payne, S. (2001). Observational study of the effect of patient-centeredness and positive approach on outcomes of general practice consultations. British Medical Journal, 323(2001), pp. 908–911.
Lohr, K. N. (Ed.). (1990). Medicare: A Strategy for Quality Assurance (Vol. 1). National Academies Press
Looney, R. (2004). Saudization and Sound Economic Reforms: Are the Two Compatible? Strategic Insights, 3 (2)
Luna, L. (1998). Culturally competent health care: A challenge for nurses in Saudi Arabia. Journal of Transcultural Nursing, 9(2), pp. 8-14.
Lynn, M. R., McMillen, B. J. and Sidani, S. (2007). Understanding and measuring patients’ assessment of the quality of nursing care. Nursing Research, 56(3), pp. 159–166.
Lyratzopoulos, G., Elliott, M., Barbiere, J. M., Henderson, A., Staetsky, L., Paddison, C., Roland, M. (2012). Understanding ethnic and other socio-demographic differences in patient experience of primary care: evidence from the English General Practice Patient Survey. BMJ Quality and Safety, 21(1), pp. 21–29.
Mahfouz, A. A., al-Sharif, A. I., el-Gamal, M. N. and Kisha, A. H. (2004). Primary health care services utilization and satisfaction among the elderly in Asir region, Saudi Arabia. Eastern Mediterranean Health Journal,10(3), pp. 365-371.
Mainz, J. (2003). Defining and classifying clinical indicators for quality improvement. International Journal for Quality in Health Care. 15, pp. 523–30.
Mallinger, J., Griggs, J. and Shields, C. (2005). Patient-centred care and breast cancer survivors’ satisfaction with information. Patient Education and Counseling, 57(3), pp.342-349.
Mann, C. and Stewart, F. (2000). Internet Communication and Qualitative Research: A Handbook for Researching Online. London. Sage.
Mansour, A. A. and Al-Osaimi, M. H. (1993).A study of satisfaction among primary health care patients in Saudi Arabia. Journal for Community Health, 18, pp. 163-173.
Mansour, A. A. and Al-Osimy, M. (1996).A study of health centres in Saudi Arabia. International Journal of Nursing Studies, 33(3), pp. 309-315.
Marshall, M. N. (1996). Sampling for qualitative research. Family Practice,13(6), pp. 522-526.
Mason, J. (2006). Qualitative Researching. 2nd ed. London: Sage.
Maxcy, S. J. (2003). Pragmatic threads in mixed methods research in the social sciences: The search for multiple modes of inquiry and the end of the philosophy of formalism. In Tashakkori, A. and Teddlie, C., eds. Handbook of Mixed Methods in Social and Behavioural Research. Thousand Oaks, CA: Sage, pp. 51–89.
May, K. A. (1991). Interview techniques in qualitative research: Concerns and challenges. Qualitative nursing research: A contemporary dialogue, 188-201.
Maynard, M. (1994). Methods, practice and epistemology: The debate about feminism and research. In Maynard, M. and Purvis, J., eds. Researching women's lives from a feminist perspective. London: Taylor and Francis, pp.10-27.
Mays, N., Pope, C., & Popay, J. (2005). Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. Journal of health services research & policy, 10(suppl 1), 6-20.
McBride, D. (2008). Blood test for breast cancer introduced in the Middle East. Oncology Nursing Society Connect. 23(6), p. 9.
McCormack L. A., Treiman, K., Rupert, D., Piehota, P. W. and Nadler, E. et al., (2011). Measuring patient-centred communication in cancer care: A literature review and the development of a systematic approach. Social Science and Medicine. 72, pp. 1085-1095.
McCormack, B. (1992). How to promote quality of care and preserve patient autonomy. British journal of nursing (Mark Allen Publishing), 2(6), 338-341.
McCormack, B. (2003). A conceptual framework for person‐centred practice with older people. International Journal of Nursing Practice, 9(3), pp.202-209.
McIlfatrick, S., Sullivan, K. and Mckenna, H. (2006). Exploring the ethical issues of the research interview in the cancer context. European Journal of Oncology Nursing. 10(1), pp. 39-47.
McWilliam, C. L., Brown, J. B. and Stewart, M. (2000). Breast cancer patients’ experiences of patient–doctor communication: A working relationship. Patient Education and Counseling. 39(2–3), pp.191-204.
Mead, M. and Bower, P. (2000). Patient-centeredness: A conceptual framework and review of the empirical literature. Social Science and Medicine. 51(7), pp 1087-1110.
Mendick, N., Young, B., Holcombe, C., and Salmon, P. (2010). The ethics of responsibility and ownership in decision-making about treatment for breast cancer: Triangulation of consultation with patient and surgeon perspectives. Social Science and Medicine, 70(12), pp.1904-1911.
Merckaert, I., Libert, Y., Messin, S., et al. (2010). Cancer patients' desire for psychological support: Prevalence and implications for screening patients' psychological needs. Psychooncology. 19, pp. 141–149.
Merkouris, A., Papathanassoglou, E. D. E. and Lemonidou, C. (2004). Evaluation of patient satisfaction with nursing care: Quantitative or qualitative approach? International Journal of Nursing Studies. 41(4), pp. 355-367.
Mertler, C. A., and Vannatta, R. A. (2010). Advanced and multivariate statistical methods: Practical application and interpretation (4th ed.). Los Angeles, CA: Pyrczak.
Michie, S., Miles, J. and Weinman, J. (2003). Patient-centeredness in chronic illness: What is it and does it matter? Patient Education and Counselling. 51, pp. 197-206.
Middelboe, T., Schjødt, T., Byrsting, K., and Gjerris, A. (2001). Ward atmosphere in acute psychiatric in‐patient care: patients' perceptions, ideals and satisfaction. Acta Psychiatrica Scandinavica, 103(3), pp. 212-219.
Miles, M. and Huberman, M. (1994). Qualitative Data Analysis: A Sourcebook of New Methods, 2. Beverly Hills, CA: Sage Publications.
Miller-Rosser, K., Chapman, Y., and Francis, K. (2006). Historical, cultural, and contemporary influences on the status of women in nursing in Saudi Arabia. Online Journal of Issues in Nursing, 11 (3)
Ministry of Health (MOH) (2001) Health statistical yearbook.Kingdom of KSA
Ministry of Health (MOH) (2010). Kingdom of Saudi Arabia: The National eHealth Program
Ministry of Labour of the Kingdom of Saudi Arabia (2009).Saudi Employment Strategy (Riyadh)
Ministry of Planning (2002b). Saudi Arabia, Achievements of the Development Plans 1970-2001, Facts and Figures, Riyadh, Ministry of Planning, No. 21
Mobeireek, A. F., Al-Kassimi, F. A., Al-Majid, S. A. and Al-Shimemry, A. (1996). Communication with the seriously ill: Physicians’ attitudes in Saudi Arabia. Journal of Medical Ethics. 22(5), pp. 282-285.
Mobeireek, A. F., Al-Kassimi, F. F., Al-Zahrani, K. K., Al-Shimemeri, A. A., Al-Damegh, S. S., Al-Amoudi, O. O. and Gamal-Eldin, M. M. (2008). Information disclosure and decision-making: The Middle East versus the Far East and the West. Journal of Medical Ethics. 34(4), pp. 225-229.
Moret, L., Nguyen, J-M., Volteau, C., Falissard, B., Lombrail, P. and Gasquet, I. (2007). Evidence of a non-linear influence of patient age on satisfaction with hospital care. International Journal of Quality Health Care,19(6), pp.382–389.
Morgan, D. L. (2007). Paradigms lost and pragmatism regained: Methodological implications of combining qualitative and quantitative methods. Journal of Mixed Method Research,1(1), pp. 48-76.
Morison, M. and Moir, J. (1998). The role of computer software in the analysis of qualitative data: Efficient clerk, research assistant or Trojan horse? Journal of Advanced Nursing. 28(1), pp. 106-116.
Muswazi, M. and Nhamo, E. (2013). Note taking: a lesson for novice qualitative researchers. Journal of Research and Method in Education, 2 (3) pp.13-17.
Needleman, J., Buerhaus, P., Mattke, S., Stewart, M., and Zelevinsky, K. (2002). Nurse-staffing levels and the quality of care in hospitals. New England Journal of Medicine, 346(22), pp. 1715-1722.
Neuman, W., L. (2003). Social Research Methods: Qualitative and Quantitative Approaches (5th ed.). Boston: Allyn and Bacon
Nguyen, T. P. L., Briançon, S., Empereur, F. and Guillemin, F.( 2002). Factors determining inpatient satisfaction with care. Social Science and Medicine. 54(4), pp. 493-504.
NHS Quality Improvement Scotland (NHS QIS 2005).Accessed online 13 July 2015 from http://www.bgs.org.uk/index.php/clinical-effectiveness/842-clineffectivenessintro
Nichols, W., Al-Amoudi, A. M., Banjar, H., Yousuf, S. A. (2013). A proposed health needs assessment to breast cancer service development in Saudi Arabia: Preparation of patient-centred tool. Life Science Journal. 10 (1), pp.463-468.
Nichols, W., Banjar, S. M. A. A. H., and Yousuf, S. A. (2013). A proposed Health Needs Assessment approach to breast cancer service development in Saudi Arabia: Preparation of a patient-centred tool. Life Science Journal, 10 (1), pp. 463-468
Novick, G. (2008). Is there a bias against telephone interviews in qualitative research? Research in Nursing and Health, 31(4), pp. 391-398.
Nursing and Midwifery Council (NMC) (2010). Standard for pre-registration nursing education. Available from: http://standards.nmc-uk.org/Pages/Welcome.aspx. [Accessed on January 2015]
Oberst, M. (1984). Patient perceptions of care: Measurements of quality and satisfaction. Cancer. 53(10), pp. 2366-2373.
Obtel, M., el-Achhab, K., Bendahhou, A., Benider, H., Errihani, A., Zidouh, R. and Bekkali, C. (2012). Measuring patient satisfaction in Moroccan oncology institutions: EORTC IN-Patsat32 and satisfaction in Moroccan patient with cancer. African Journal of Cancer, 4(1), pp.9-17.
Ommen, O., Wirtz,M., Janssen,C., Neumann, M., Ernstmann, N. and Pfaff, H. (2010). Validation of a theory-based instrument measuring patient-reported psychosocial care by physicians using multiple indicators and multiple causes model. Patient Education and Counselling, 80 (1), pp.100-6.
Ong, L. M. L., de Haes J. C. J. M., Hoos, A. M. and Lammes, F. B. (1995). Doctor-patient communication: A review of the literature. Social Science and Medicine. 40(7), pp. 903-918.
Ong, L. M. L., Visser, M. R. M., Lammes F. B. and de Haes J. C. J. M. (2000). Doctor–patient communication and cancer patients’ quality of life and satisfaction. Patient Education and Counselling. 41(2), pp. 145-156.
Onwuegbuzie, A. and Johnson, B. (2004). Mixed methods research: A research paradigm whose time has come. Educational Researcher, 33(7), pp.14-26.
Onwuegbuzie, A. J. and Leech, N. L. (2006). Linking research questions to mixed methods data analysis procedures. The Qualitative Report, 11(3), pp. 474-498.
Onwuegbuzie, A. J., Leech, N. L. (2005). Taking the "Q" out of research: Teaching research methodology courses without the divide between quantitative and qualitative paradigms. Quality and Quantity, 39(3), pp. 267-296.
Opdenakker, R. (2006). Advantages and disadvantages of four interview techniques in qualitative research. Qualitative Social Research. 7(4), ISSN 1438-5627 Available at: <http://www.qualitative-research.net/index.php/fqs/article/view/175>. [Date accessed: 01 Mar. 2015].
Parahoo, K. (2006). Nursing Research: Principles, Process and Issues. 2nd ed. Basingstoke: Palgrave Macmillan.
Parker, P., Baile, W., de Moor, C. and Cohen, L. (2003). Psychosocial and demographic predictors of quality of life in a large sample of cancer patients. Psych-oncology. 12 (2), pp.183-93.
Parkin, D. M. and Fernandez, L. M. (2006). Use of statistics to assess the global burden of breast cancer. The Breast Journal, 12(s1), pp. S70-S80.
Pascoe, G. C. (1983). Patient satisfaction in primary health care: a literature review and analysis. Evaluation and Program Planning, 6(3), pp. 185-210.
Patton, M. (2002). Qualitative Research and Evaluation Methods. 3rd ed. Thousand Oaks, CA: Sage.
Payne, S., Jarrett, N., Jeffs, D. and Brown, L. (2001). Implications of social isolation during cancer treatment: The implications of residence away from home during cancer treatment on patients’ experiences: a comparative study. Health and Place. 7(4), pp. 273-282.
Pishkuhi, M. A., Salmaniyan, S., Nedjat, S., Zendedel, K., and Lari, M. A. (2014). Psychometric Properties of the Persian Version of Satisfaction with Care EORTC-in-patsat32 Questionnaire among Iranian Cancer Patients. Asian Pacific Journal of Cancer Prevention, 15(23), 10121-10128.
Plaza, D. P., Soriano, E. and Higginbottom, G. (2013). Sociocultural and linguistic boundaries influencing intercultural communication between nurses and Moroccan patients in southern Spain: A focused ethnography. BMC Nursing. 12(1), pp. 14.
Polit, D. and Beck, C. (2006). Essentials of Nursing Care: Methods, Appraisal and Utilization. 6th ed. Philadelphia: Lippincott Williams and Wilkins.
Polit, D. and Hungler, B. (2001). Nursing Research: Principles and Methods. Lippincott: Philadelphia.
Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M. and Duffy, S. (2006). Guidance on the conduct of narrative synthesis in systematic reviews: A product from the ESRC Methods Programme. Lancaster.
Pope, C. and Mays, N. (1995). Qualitative Research: Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ, 311, pp. 42-45.
Pope, C., Van Royen, P., and Baker, R. (2002). Qualitative methods in research on healthcare quality. Quality and Safety in Health Care, 11(2) pp.148-152.
Pope, C., Ziebland, S. and Mays, N. (2000). Qualitative research in health care: Analysing qualitative data. British Medical Journal. 320(7227), pp. 114–6.
Quintana, J. M., González, N., Bilbao, A., Aizpuru, F., Escobar, A., Esteban, C. and Thompson, A. (2006). Predictors of patient satisfaction with hospital health care. BMC Health Service Research, 6 (1)102.
Rafii, F., Hajinezhad, M. and Haghani, H. ( 2008). Nurse caring in Iran and its relationship with patient satisfaction. Australian Journal of Advanced Nursing,26(2), pp. 75-84.
Rahmqvist, M. (2001). Patient satisfaction about age, health status and other background factors: A model for comparisons of care units. International Journal for Quality in Health Care. 13, pp. 385-90.
Rahmqvist, M. and Bara, A. (2010) Patient characteristics and quality dimensions related to patient satisfaction. International Journal for Quality in Health Care. 22(2), pp. 86-92.
Rao, J.K., Anderson, L.A., Inui, T.S. and Frankel, R.M. (2007). Communication interventions make a difference in conversations between physicians and patients: a systematic review of the evidence. Medical Care, 45 (4) pp.340-349.
Rao, K., Peters, D. and Bandeen-Roche, K. (2006). Towards patient-centred health services in India: A scale to measure patient perceptions of quality. International Journal for Quality in Health Care, 18(6), pp. 414-421.
Rashad, A., MacVane Phipps, F. and Haith-Cooper, M. (2004). Obtaining informed consent in Egyptian research study. Nursing Ethics, 11(4), pp. 394-399.
Rastogi, T., Hildesheim, A. and Sinha, R. (2004). Opportunities for cancer epidemiology in developing countries. Nature Reviews Cancer, 4 (11), pp. 909‐17
Rchaidia, L., Dierckx de Casterlé, B., De Blaeser, L., Gastmans, C. (2009). Cancer patients' perceptions of the good nurse: A literature review. Nursing Ethics. 16(5), pp. 528-542.
Rhemtulla, M. and Little, T. (2012). Tools of the trade: Planned missing data designs for research in cognitive development. Journal of Cognitive Development. 13(4). Available online from: < http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3857527/ >. [Retrieved 10 Jan 2015].
Richards, L. (1999). Using NVivo in Qualitative Research. London: Sage.
Richards, L. (2009). Handling Qualitative Data. 2nd ed. London: Sage.
Ritchie J and Lewis J (2003). Qualitative research practice: a guide for social science students and researchers London, Sage Publication.
Rodgers, M., Sowden, A., Petticrew, M., Arai, L., Roberts, H., Britten, N. and Popay, J. (2009). Testing methodological guidance on the conduct of narrative synthesis in systematic reviews: Effectiveness of interventions to promote smoke alarm ownership and function. Evaluation. 15(1), pp. 49-73.
Rosman, S.(2004). Cancer and stigma: Experience of patients with chemotherapy-induced alopecia. Patient Education and Counseling, 52 (3), pp. 333–339.
Rossberg, J. I., Melle, I., Opjordsmoen, S., and Friis, S. (2006). Patient satisfaction and treatment environment: A 20-year follow-up study from an acute psychiatric ward. Nordic Journal of Psychiatry, 60(2), pp.176-180.
Roter, D. (2000). The enduring and evolving nature of the patient-physician relationship. Patient Education and Counselling, 39 (1), pp. 5-15.
Rothman, K. and Greenland, S. (1998). Modern Epidemiology. 2nd ed. Philadelphia: Lippincott-Raven.
Rowlands, J. and Noble, S. (2008). How does the environment impact the quality of life of advanced cancer patients? A qualitative study with implications for ward design. Palliative Medicine. 22(6), pp. 768-774.
Rubin, H. and Rubin, I. (1995). Qualitative Interviewing: The Art of Hearing Data. Thousand Oaks, CA: Sage.
Saeed, A. A. and Mohamed, B. A. (2002). Patient's perspective on factors affecting utilization of primary health care centres in Riyadh, Saudi Arabia. Saudi Medicine Journal, 23(10), pp.1237-42.
Sait, K. H., Anfinan, N. M., Eldeek, B., Al-Ahmadi, J., Al-Attas, M., Sait, H. K., Basalamad, H. A., Al-Ama, N., and El-Sayed, M. E. (2014). Perceptions of patients with cancer towards support management services and use of complementary alternative medicine- a single institution hospital-based study in Saudi Arabia. Asian Pacific Journal of Cancer Prevention, 15 (6), pp. 2547-2554.
Sale, J., Lohfeld, L., Brazil, K. (2002). Revisiting the quantitative-qualitative debate: Implications for mixed methods research. Quality and Quantity, 36(1), pp. 43–53.
Sands, R., Bourjolly, J. and Roer-Strier, D. (2007). Crossing cultural barriers in research interviewing. Qualitative Social Work, 6(3), pp. 353-372.
Sanson-Fisher, R., Girgis, A., Boyes, A., Bonevski, B., Burton, L., Cook, P. (2000). The unmet supportive care needs of patients with cancer. Supportive Care Review Group. Cancer. 88, pp. 226–37.
Saudi Cancer Registry (2010) Cancer Incidence Report 2010, Council of Health services, Kingdom of Saudi Arabia [Accessed online] on 1st October 2015 from
http://www.chs.gov.sa/Ar/mediacenter/NewsLetter/2010%20Report%20(1).pdf
Scotland Office for National Statistics (2014) Registrar General’s annual review of demographic trends. A national statistics publication for Scotland [Accessed online from] http://www.nrscotland.gov.uk/files/statistics/annual-review-2012/rgar-2012.pdf
Scott, T., Mannion, R., Davies, H. T. O. and Marshall, M. N. (2003). Implementing culture change in health care: Theory and practice. International Journal for Quality in Health Care. 15(2), pp. 111-118.
Serhier, Z., Obtel, M and Bendahhou, K. (2011) Adaptation transculturelle et validation du questionnaire EORTC IN-PATSAT32 chez les patients marocains atteints de cancer. Bull Cancer (submitted)
Shamieh, O., al-Shehri, R. and el-Foudeh, M. (2010). Access to Palliative Care: Initiative to Improve Cancer Care in the Arab World. Riyadh: National Guard Health Affairs.
Shattell, M. (2004). Nurse-patient interaction: A review of the literature. Journal of Clinical Nursing. 13, pp. 714-722.
Shaw, B. R., Han, J. Y., Hawkins, R. P., Stewart, J., McTavish, F. and Gustafson D. H. (2007). Doctor–patient relationship as motivation and outcome: Examining uses of an interactive cancer communication system. International Journal of Medical Informatics. 76, pp. 274-282.
Shuldham, C., Parkin, C., Firouzi, A., Roughton, M. and Lau-Walker, M. (2009). The relationship between nurse staffing and patient outcomes: A case study. International Journal of Nursing Studies. 46(7), pp. 986-992.
Silbermann, M. and Hassan, E. (2011).Cultural perspectives in cancer care: Impact of Islamic traditions and practices in Middle Eastern countries. Journal of Pediatric Hematology Oncology. 33, pp. S81-S86.
Silverman, D. (2013). Doing Qualitative Research: A Practical Handbook. London: Sage.
Singh, J. (1989). The patient satisfaction concept: a review and reconceptualization. Adv Consum Res, 16, 176-9.
Siourouni, E., Kastanioti, C., Tzialla, Dand Niakas, D. (2012) Health care provider’s organizational culture profile: a literature review. Health Science Journal, 6 (2) p.212-233
Sitzia, J. and Wood, N. (1997). Patient satisfaction: a review of issues and concepts. Social Science & Medicine, 45(12), pp.1829-1843.
Sitzia, J. and Wood, N. (1998). Patient satisfaction with cancer chemotherapy nursing: a review of the literature. International Journal of Nursing Studies, 35, pp. 1-12.
Sizmur,S.and Redding,D (2009). Core domains for measuring inpatients’ experience of care. Picker Institute Europe
Smith, C. (1992). Validation of a patient satisfaction system in the United Kingdom. Quality Assurance in Health Care, 4(3), pp.171-177.
Snape, D. and Spencer, L. (2003). The foundations of qualitative research. In Ritchie, J. and Lewis, L., eds. Qualitative Research Practice: A Guide for Social Science Students and Researchers. Los Angeles: Sage, pp. 1-23.
Snilstveit, B., Oliver, S., and Vojtkova, M. (2012). Narrative approaches to systematic review and synthesis of evidence for international development policy and practice Journal of Development Effectiveness. 4(3), pp. 409-429.
Sofaer, S. and Firminger, K. (2005). Patient perceptions of the quality of health services. Annual Review of Public Health, 26, pp. 513–559.
Sokol, D. (2006). How the doctor's nose has shortened over time: A historical overview of the truth-telling debate in the doctor-patient relationship. Journal of the Royal Society of Medicine. 99(12), pp. 632-636.
Stavropoulou, C. (2010). Non-adherence to medication and doctor-patient relationship: Evidence from a European survey. Patient Education and Counseling, 83 (1), pp. 7-13.
Stewart, M.(2001). Toward a global definition of patient-centred care: The patient should be the judge of patient-centred care. BMJ, 322(7284), pp. 444-445.
Stewart, W., Shamdasani, P. and Rook, D. (2007). Focus Group: Theory and Practice. 2nd ed. Thousand Oaks, CA: Sage.
Strauss, A. and Corbin, J. (2008). Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. 3rd ed. Thousand Oaks, CA: Sage.
Street, R., Makoul, G., Arora, N. and Epstein, R. (2009). How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Education and Counselling, 74(3), pp. 295-301.
Sturges, J. E. and Hanrahan, K. J. (2004). Comparing telephone and face-to-face qualitative interviewing: A research note. Qualitative Research, 4(1), pp. 107-118.
Tanaka, A., Iwamoto,T., Kaneyasu, H. and Petrini, A. (1999). Thoughts and feelings of in-patients with advanced terminal cancer: Implications for terminal care improvement. Nursing and Health Sciences. 1(3), pp.189-193.
Tarlov, A. R., Ware, J. E., Greenfield, S., Nelson, E. C., Perrin, E., and Zubkoff, M. (1989). The Medical Outcomes Study: an application of methods for monitoring the results of medical care. JAMA, 262(7) pp. 925-930
Tashakkori, A. and Teddlie, C. (1998). Mixed Methodology: Combining Qualitative and Quantitative Approaches. Thousand Oaks, CA: Sage.
Tashakkori, A. and Teddlie, C., eds. (2003). Handbook on Mixed Methods in the Behavioral and Social Sciences. Thousand Oaks, CA: Sage.
Teddlie, C. and Yu, F. (2007). Mixed methods sampling. Journal of Mixed Methods Research. 1(1), pp. 77-100.
Temple, B. (1997). Watch your tongue: Issues in translation and cross-cultural research. Sociology, 31(3), pp. 607-618.
Thorne, S., Oliffe, J., Stajduhar, K., Oglov, V., Kim-Sing, C. and Hislop, T. (2013). Poor communication in cancer care: Patient perspectives on what it is and what to do about it. Cancer Nursing, 36 (6), pp. 445-453
Timko, C., and Moos, R. H. (1998). Outcomes of the treatment climate in psychiatric and substance abuse programs. Journal of Clinical Psychology, 54(8), pp.1137-1150.
Tsianakas, V., Maben, J., Wiseman, T., Robert, G., Richardson, A., Madden, P., ... & Davies, E. A. (2012). Using patients’ experiences to identify priorities for quality improvement in breast cancer care: patient narratives, surveys or both? BMC health services research, 12(1), 271.
Tuli, F. (2011). The basis of the distinction between qualitative and quantitative research in social science: reflection on ontological, epistemological and methodological perspectives. Ethiopian Journal of Education and Sciences, 6(1) pp.97-108
Tumulty, G. (2001). Professional development of nursing in Saudi Arabia. Journal of Nursing Scholarship, 33(3), pp.285-290.
Turhal, N. S., Efe, B., Gumus, M., Aliustaoglu, M., Karamanoglu, A. and Senoz, M. (2002). Patient satisfaction in the outpatients’ chemotherapy unit of Marmara University, Istanbul, Turkey: A staff survey. BMC Cancer, 2(30). Available online from: <http://www.biomedcentral.com/1471-2407/2/30>.
Turris, S. A. (2005). Unpacking the concept of patient satisfaction: A feminist analysis. Journal of Advanced Nursing, 50(3), pp. 293-8.
Tzeng, H., Ketefian, S. and Redman, R. W. ( 2002). Relationship of Nurses’ assessment of organizational culture, job satisfaction, and patient Satisfaction with Nursing care. International Journal of Nursing Studies. 39(1), pp. 79-84.
Ulrich, R., Zimring, C., Joseph, A. and Choudhary, R. (2004).The role of the physical environment in the hospital of the 21st century: A once-in-a-lifetime opportunity. Report to the Center for Health Design for the “Designing the 21st Century Hospital Project”. Concord, CA: The Center for Health Design.
Valsecchi, M. G. and Steliarova‐Foucher, E. (2008). Cancer registration in developing countries: Luxury or necessity? Lancet Oncology. 9(2), pp. 159-67.
Vermeire, E., Hearnshaw, H., Van Royen, P., Denekens, J. (2001). Patient adherence to treatment: three decades of research- A comprehensive review. Journal of Clinical Pharmacology Therapy, 26 (3), pp. 331-342.
Vos, M., Graafmans, W., Kooistra, M., Mmijboo, B., Voort, P. V. and Westert, G. (2009). Using quality indicators to improve hospital care: A review of the literature. International Journal for Quality in Health Care, 21(2), pp. 119-129.
Wagner, D. and Bear, M. ( 2009). Patient satisfaction with nursing care: A concept analysis within a nursing framework. Journal of Advanced Nursing, 65(3), pp. 692-701.
Walker, L. (2009).The right to health in Saudi Arabia: 'Right to health in the Middle East project'. University of Aberdeen, School of Law Report. Available online from: <http://www.abdn.ac.uk/law/hhr.shtml>.
Walliman, N. (2005). Your Research Project: A Step-By-Step Guide for the First Time Researcher. 2nd ed. London: Sage.
Walston, S., Al-Harbi, Y., and Al-Omar, B. (2008). The changing face of healthcare in Saudi Arabia. Annals of Saudi Medicine, 28 (4), 243-250.
Ware, J. E., and Davis, A. R. (1983). Behavioural consequences of consumer dissatisfaction with medical care. Evaluation and program planning, 6(3) pp.291-297.
Ware Jr, J. E. and Hays, R. D. (1988). Methods for measuring patient satisfaction with specific medical encounters. Medical care, 26(4), pp.393-402.
Ware, J. E., Snyder, M. K., Wright, R. and Davies, A. E. (1983). Defining and measuring patient satisfaction with medical care. Evaluation and Programme Planning, 6 (3), pp. 247-263.
Weber, A.S., Verjee, M. A., Musson, D., Iqbal, N. A., Mosleh, T. M., Zainel, A. A., and Al-Salamy, Y. (2011). Patient opinion of the doctor-patient relationship in public hospitals in Qatar. Saudi Medical Journal, 32 (3), pp. 293-299.
Wengraf, T. (2001). Qualitative research interviewing: Biographic narrative and semi-structured methods. Sage.
Westaway, M. S., Rheeder, P., Van Zyl, D. G., and Seager, J. R. (2003). Interpersonal and organizational dimensions of patient satisfaction: the moderating effects of health status. International Journal for Quality in Health Care, 15(4), pp.337-344.
Wildes, K., Miller, A., San Miguel, S., Otto, M. and Ramirez, A.(2011). The satisfaction of Latina breast cancer survivors with their healthcare and health-related quality of life. Journal of Women's Health, 20(7), pp. 1065-1074.
Williams B. (1994). Patient satisfaction: A valid concept? Social Science and Medicine, 38(4), pp. 509-516.
Williams, B., Coyle, J. and Healy, D. (1998). The meaning of patient satisfaction: An explanation of high reported levels. Social Science and Medicine, 47(9), pp.1351-1359.
Williams, S. J. and Calnan, M. (1991). Key determinants of consumer satisfaction with general practice. Journal of Family Practice, 8 (3), pp. 237-242.
Williamson, M. and Harrison, L. (2010). Providing culturally appropriate care: A literature review. International Journal of Nursing Studies, 47 (6), pp. 761–769.
Wolf, D. M., Lehman, L., Quinlin, R., Zullo, T., & Hoffman, L. (2008). Effect of Patient‐Centered Care on Patient Satisfaction and Quality of Care. Journal of Nursing Care Quality, 23(4), 316-321.
World Health Organization (WHO) (2009). Towards a strategy for cancer control in the Eastern Mediterranean region. Available online from: <http://www.emro.who.int/dsaf/dsa1002.pdf>. [Accessed 20 September, 2011].
World Health Organization, WHO (2008).The World Health Report 2008: primary health care - now more than ever. Geneva
World Population Review (2014). Available online from: <http://worldpopulationreview.com/countries/saudi-arabia-population/>.
Younge, D., Moreau, P., Ezzat, A., Gray, A. (1997). Communicating with cancer patients in Saudi Arabia. Annals of New York Academy of Science. 809 (1), pp. 309–316.
Zahl, P. H., Maehlen, J. and Welch, H. G. (2008). The natural history of invasive breast cancers detected by screening mammography. Archives of Internal Medicine. 168 (21), pp. 2311-6.
Zhao, S. H., Akkadechanunt, T. and Xue, X. L. ( 2009). Quality nursing care as perceived by nurses and patients in a Chinese hospital. Journal of Clinical Nursing. 18(12), pp. 1722-1728.
Appendices
Appendix1: Percentage Distribution of Cancer Incidence among Saudis by Sex according to Age Group, 2010 (Saudi Cancer Registry 2010)
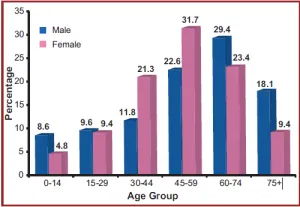
Appendix 2: Search and screening process
Databases search date: 07-01-2014
Databases | Search terms | Results |
Science Direct Limiters: ● Published Date: 1980 -2014 ● English Language Boolean operator AND, OR | patient satisfaction, quality of care patient satisfaction, Saudi Saudi patient satisfaction, quality of care Saudi Cancer, patient satisfaction, quality care quality health care, Saudi communication, Saudi, quality of care | 4969 papers returned 100 papers returned 38 papers returned 467 papers returned 177 papers returned 219 papers returned |
CINAHL Limiters FOR CINAHL : ● Published Date: 1980 -2014 ● English Language ● Peer Reviewed ● Language: English ● Inpatients Boolean operator: AND, OR | patient satisfaction, quality of health care patient satisfaction, Saudi quality of health care, Saudi doctor communication skills, Saudi | 38 papers returned 1 paper returned 29 papers returned 53 papers returned |
Web of Science (including Medline) Limiters: ● Published Date: 1980 -2014 ● English Language Boolean operator: AND, OR | patient satisfaction, Saudi communication, Saudi cancer care patient satisfaction, Saudi hospital quality care cancer patient satisfaction, Saudi | 163 papers returned 14 papers returned 36 papers returned 5 paper returned |
Google Scholar Limiters: · Published date: 1980-2014 · English language Boolean operator: AND, OR | patient satisfaction, Saudi, quality care, patient-centred care, oncology, hospitals, doctor-patient communication | 2500 papers returned |
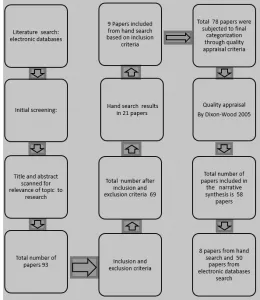
Appendix 3: Inclusion and exclusion criteria of the literature search strategy
Inclusion criteria | Exclusion criteria |
1. Research papers that were found in peer-reviewed journals or referenced government/non-government publications were included. | 1. Papers that were limited to the outcomes of cancer treatment drugs or symptom management were excluded. |
2. Studies based on KSA that had investigated the quality of hospital care for patients in general and cancer care patients in particular were included and only adult cancer patient's studies were included for the focus of this review. | 2. Studies investigating the quality of hospital care for non-adult patients with or without cancer were excluded. |
3. Those studies that had used review, qualitative, quantitative or mixed approaches were included. | 3. Studies not supported by peer-reviewed journals were excluded. |
4. Studies conducted between 1980 and 2014 were included. | |
5. Research that examined patient satisfaction using either of the factors of measurements, patient-centred care, doctor-patient relationship, structure of healthcare delivery system, disclosure practices, and gender inequality were considered and included in the literature review. Other literature included examined the impact of patient satisfaction as a basis for theoretical arguments for the current study even if the study was not based on KSA. |
Appendix 4: Criteria for quality appraisal of chosen studies in literature review
Quality appraisal criteria by Dixon-Woods et al. (2005)
- Are the aims and objectives of the research clearly stated?
- Is the research design specified and appropriate for the aims and objectives of the research?
- Do the researchers provide a clear account of the process by which their findings were produced?
- Do the researchers display enough data to support their interpretation and conclusions?
- Is the method of analysis appropriate and adequately explicated?
One point was given for each of the above, and studies that conformed to 3 out of 5 were selected for review.
Appendix 5: Table of included studies
| Author-date | Sample | Methods | Key findings | Comments |
1 | Alaloola & AlBedawi (2008) Patient satisfaction in a Riyadh tertiary care centre. International Journal of Health Care Quality Assurance. vol. 21, no7, 2008 | 1983 inpatients, outpatients and ER patients | Cross-sectional survey Using a self-developed patient satisfaction questionnaire | Patient satisfaction was noted in environmental aspects - room temp—etc. and less found in inter interpersonal skills of doctors, and phlebotomists, as they failed to introduce themselves. | · Lack of clarity in describing the tool they used –like question areas. · The focus of the satisfaction domain was only in the socio-demographic context. · No focus on specific services such as cancer, or medical, which is a limitation · Although it is valuable for originality, further research is needed in the cancer setting in the KSA |
2 | Al-Doghaither & Saeed A. A. (2000) Consumers' satisfaction with primary health services in the city of Jeddah, Saudi Arabia. | 75 patients aged over 15 years, chosen systematically | Self- Self-administered questionnaire pilot test | Satisfaction scores were higher in those taking consideration of all services, while individual components of the service were scored less. | · Although high scores for satisfaction were noticed, the service component needs to be monitored too and assessed to provide satisfactory services |
3 | Saeed & Mohamad (2002) Satisfaction and correlates of patients' satisfaction with physicians' services in primary health care centres By Saudi Medical Journal | n=540 patients in 8 PHC, selected randomly in Riyadh | Survey questionnaire, pilot-tested | Service items need to have the correct measure Also, young and adult patients need more attention | · No clear description of recruitment and methods -Other domains like hospital services, and nurses’ skills would have an impact on the satisfaction level of patients |
4 | Al-Ahmadi & Roland, M. (2005) Quality of primary health care in Saudi Arabia: A comprehensive review. | A systematic review of 31 papers met the inclusion | Reviews of literature | There were variations in the quality of primary health care services in the KSA More effort is needed in the management and organisation of these services | · Further research is needed to address quality concerns from the patient’s perspective to have better insight into quality care |
5 | Mahfouz et al. (2004) Primary health care services utilisation and satisfaction among the elderly in Asir region, Saudi Arabia | 253 patients | In 26 PHC in ASIR (6 urban and 20 rural centres), a House-to-house survey by an interview with an expert health worker, and Arabic speaker, to answer survey questions The questionnaire addresses 5 aspects of services adopted from Mansour and Al-Osaimi's study 1993 (continuity of care, humanity, accessibility, thoroughness and information). | Satisfied patients reported but 79% dissatisfaction found in 3 items: lack of audio-visual for patient education, lack of enough speciality clinics and prolonged waiting time in centres. | · More information is needed regarding the tools used · Emphasis on 5 aspects of lack of reasoning · More concerns are needed in evaluating different socio-demographic characteristics in elderly patients - results will be significantly different from area to area so such a comparison would be desirable |
6 | Akhtar & Nadrah (2005) Assessment of the quality of breast cancer care: A single institutional study from Saudi Arabia | 78 operable breast cancer patient | Retrospective analysis of breast cancer patient charts and histopathology reports from 1995-2000 | Only 37% had triple assessment before surgical procedure radiotherapy not used as per the required standard The overall conclusion is that quality is below international standard |
|
7 | Ibrahim et al. (2002) Appraisal of communication skills and patients' satisfaction in cross-language encounters in oncology practice. | 255 patients | Questionnaire “Art of Medicine” used to assess patients' perceptions of clinicians' communication behaviours and patients' global satisfaction. | No difference - means that language doesn’t affect interpersonal skills like communication and patient satisfaction. Patients were equally satisfied in both languages. | · Interesting finding but the scale used was not described clearly. · Further research is needed to evidence that cross-language communication is not a barrier to patient satisfaction within the multi-dimensional needs of cancer patients and cultural differences |
8 | Alahwal et al. (1998) “Cancer patients’ awareness of their disease and prognosis”, Annals of Saudi Medicine, Vol. 18 No. 2, pp. 187-9. | 136 (33 cancer patients, 63 doctors, and 40 laypeople) | A questionnaire of 4 questions was developed for this study Distributed in the western region of Saudi Arabia (major hospital providing cancer care) | All patients were in favour of being given full information regarding cancer; this would help them have a better understanding of how to deal with their illness. Doctors too favoured that the patients be disclosed about their conditions. | · Although patient views were taken, the methods would be more useful had qualitative interviews been used as this provides expanded insights into communication issues with patients |
9 | Younge et al. (1997) Communicating with cancer patients in Saudi Arabia | None | By literature review on communication aspects and factors influencing communication in the KSA | Communication is influenced by many factors such as cultural and social and also health services that lack community care for chronic illness. | · Although valuable information was obtained, there was no clear methodology mentioned, also several studies reviewed were not mentioned and this generalisation potentially limits the findings. |
10 | Mansour and Al-Osimy (1996) A study of health centres in Saudi Arabia | 300 Consumers | Via assessment sheet of centres’ resources in terms of quality and availability and consumer satisfaction & a 4-point system Likert scale to measure satisfaction in 5 domains: continuity of care, accessibility, humaneness, information and thoroughness. | A discrepancy of data has been found between centres’ resources evaluation and consumer satisfaction results | · More studies are needed to evaluate resources and satisfaction through valid measures. · Studies in hospital resources can provide further insight into patient satisfaction since they focus only on health centres. |
11 Sweden | Rahmqvist and Bara (2010) Patient characteristics and quality dimensions related to patient satisfaction. | 7425 patients in all medical centres in Sweden | Questionnaire concerned with the perceived quality of healthcare | Older patients with good health status were satisfied 90% Interestingly, educated patients with poor health status were dissatisfied in comparison to less-educated patients and better health status |
|
12 | Williamson, M.J. & Harrison, L. (2010) Providing culturally appropriate care: A literature review International Journal of Nursing Studies, vol. 47, no. 6, pp. 761-769. | None | Literature review through multiple databases search | Cultural factors found to impact on health The focus was on the cognitive aspect of culture, values & beliefs, thus there was a failure to identify specific mechanisms that culture has as a negative health mechanism |
|
13 | Walston et al. (2008) The changing face of health care in Saudi Arabia | None | Review of literature | The complexity of changing the health care system in the KSA is a continuous challenge and private health care needs to be reformed to augment the needs of healthcare |
|
14 | Almuzaini et al. (1998) The Attitude of Health Care Professionals toward the availability of Hospice Services for Cancer Patients and their Carers in Saudi Arabia | 695 (398 healthcare professionals, 136 cancer patients and 161 informal carers) | A quantitative survey of participants on the quality of healthcare | There is a lack of consistency in the quality of health care in KSA. The Ministry-owned or managed facilities score poorly on patient satisfaction with service organisation. The university and the military facilities do slightly better than the government-managed facilities on patient satisfaction. |
|
15 | Elkum et al. (2007) Being 40 or younger is an independent risk factor for relapse inoperable breast cancer patients: The Saudi Arabia experience | 867 breast cancer patient data at King Faisal Specialist Hospital and Research Centre (KFSH&RC) from 1986 to 2002 were reviewed | The researchers used hospital patients’ records for collecting data. They employed statistical techniques to establish the correlation between age and breast cancer prognosis. | The research established that women under 40 were more prone to having a terminal prognosis and complexities. It also found that the treatment protocols in KSA were the same as in the USA, and hence the quality of care was good. |
|
16 | Amri and Sadat (2009) Cancer chemotherapy-induced osteoporosis: How common is it among Saudi Arabian cancer survivors | 71 patients who received chemotherapy in Saudi Arabia were examined for osteoporosis through bone scans. | 71 patients | The main findings indicated that there was a high level of risk for osteoporosis for patients treated with chemotherapy. There was a lack of standard BMD (Bone Mineral Density) testing that could lead to early detection. There was also a scarcity of drugs that could help prevent the condition |
|
17 | Brown et al. (2009) Failure to attend appointments and loss to follow-up: a prospective study of patients with malignant lymphoma in Riyadh, Saudi Arabia | A 3-year prospective study of 199 patients with malignant lymphoma in Riyadh | Retrospective analysis of No Shows appointments (No Shows=340 ) | 34% were related to hospital-based communication errors. 17.6 % were related to errors in patient communication with the hospital |
|
18 | Jazieh, A.R. (2010) Human resources development, ‘Initiative to Improve Cancer Care in the Arab World’ | 12 Experts in health care from across the Arab world and international experts | Interviews, situational analysis | There is a lack of high-quality and well-trained healthcare professionals |
|
19 | Saghir & Azim (2010) Standards of Care and Guidelines for the Arab World with Limited Resources | 12 experts in health care from across the Arab world | Panel discussions | Lack of standardisation in doctors’ and nurses’ skills leads to varying quality. |
|
20 | Diab, R. (2010) Access to Cancer Care Facilities, ‘Initiative to Improve Cancer Care in the Arab World’, | 8-panel members made of experts in policy-making, healthcare and scholars (a | Panel discussions (Based on the discussion of panel members about the priority of objectives and available baseline information of accessibility to cancer care) | The panel found that the quality of cancer care suffered from problems like long wait times for the patients, high costs, lack of access to health care and inequality in access for people from rural and marginalised regions. |
|
21 | Shamieh et al. (2010)Access to palliative care | 12 multi-disciplinary experts in palliative care | Panel discussion | Access to cancer care is poor compared to palliative care |
|
22 | Cornell, B. et al. (2009) Measuring the quality of hospital care: an inventory of indicators. Internal Medicine Journal, 39 (6), pp. 352-360. | None | Literature review | The literature review revealed that the quality indicators for measuring healthcare quality were varied and non-standardised. The researchers found over 300 indicators of quality used in the available literature. |
|
23 | Walker (2009) The right to health in Saudi Arabia | None | Review of available international and regional human development reports, independent research and newspaper articles | Social issues like the low position of women in society, and lack of social and political freedom impact the access to quality care. |
|
24 | Dein & Stygall (1997) Does being religious help or hinder coping with chronic illness? A critical literature review. | None | Literature review | The researchers found a correlation between spiritual beliefs, religious practices and psychological prognosis, and made recommendations for integrating religious empathy in health care |
|
25 | Al-Faris, E.A., Khoja, T., Falouda, M. and Saeed, A.A.W., (1996). Patients' satisfaction with accessibility and services offered in Riyadh health centres. Saudi Medical Journal, 17(1), pp. 11-17. | 466 randomly selected patients from 6 randomly selected primary health care centres PHCC in Riyadh City | Patient satisfaction and attitude survey | The research found a high level of satisfaction among older patients, housewives and non-Saudi patients. |
|
26 | Al-Sirafy, S.A., Hassan, A.A. and Al-Shahri, M.Z. (2009) Hospitalisation pattern in a hospital-based palliative care program: An example from Saudi Arabia. American Journal of Hospice and Palliative Medicine, 26(1), pp. 52-56. | 759 palliative patient admissions during 4 years (in the absence of sub-acute palliative care models) | A retrospective review of palliative admissions was studied for the reason for hospitalisation, duration of stay and mortality rate | The research found that quality of life did not improve with palliative care in Saudi Arabia. The indicators of quality for palliative care included factors like duration of stay mortality and quality of life. |
|
27 | Groene, O. et al. (2008) An international review of projects on hospital performance assessment. Int J Qual Health Care 20: 162–71. | None | Literature review, expert interviews, performance assessment tool for quality improvement in hospitals (PATH). | The research found that there was a substantial lack of standardisation in terms of quality indicators. The research could identify only 11 hospital performance measurement projects that contained standardised methodology and showed robust design. |
|
28 | Mainz J. (2003) Defining and classifying clinical indicators for quality improvement. Int J Qual Health Care, 15: pp.523–30. | None | Literature review | A review of available literature on quality indicators for health care highlighted that quality is divided into structural, process-related and outcome-related. |
|
29 Japan | Tanaka, A, et al. (1999) Thoughts and feelings of in-patients with advanced terminal cancer: Implications for terminal care improvement. Nursing & health sciences, 1(3), pp.189-193. | Eight terminally ill patients with cancer | Semi-structured Interviews | The research found that the patients wanted solutions for pain control, needed family support, and wanted to live their lives ordinarily as much as possible. The desire to do their best with what they have led them to have a positive attitude and improve their illness management. |
|
30 | McBride, D. (2008). Blood Test for Breast Cancer Introduced in the Middle East. ONS Connect, 23(6), 9. | None | Article based on independent research by the author who is a nurse at the Kaiser Permanente Oakland Medical Centre and a faculty member at Samuel Merritt College in Oakland, CA | The article discusses the introduction of blood tests in the Middle East to improve breast cancer detection |
|
31 | Aljubran, A. (2010) The attitude toward disclosure of bad news to cancer patients in Saudi Arabia. Annual Saudi Med, March April. 2010 | None | Literature review | The researchers highlight the changing trends in patients’ need to understand and know their illnesses. |
|
32 | Bredart et al. (2007) Determinants of patient satisfaction in oncology settings from European and Asian countries: Preliminary results based on the EORTC IN-PATSAT32 questionnaire. European Journal of Cancer, 43(2), 323-330. | 647 cancer patients from hospitals in the EU and Asia | EORTC INPATSAT32 Questionnaire; quality of life of the patients and socio-demographic data; institutional data. | Quality indicators found included the number of nurses and doctors per bed, size of the hospital, setting of the ward; geo-cultural origin, patient awareness; global health status, and education level |
|
33 | Linder Pelz Towards a theory of Patient satisfaction. Social Science and Medicine, 6 (1982), 577-82. | None | Review of literature | Defining and conceptualising what is patient satisfaction |
|
34 | Pascoe. (1983) Patient satisfaction in primary health care; a literature review. Evaluation and program planning, 6 3-4, 85-210. | None | Review of literature | An interpretive and reflexive review of literature on access to healthcare |
|
35 | Keith. R. (1998) Patient satisfaction and rehabilitation service. Arch Physical Medical Rehabilitation Journal.1998 (79), 1112-8 | None | Discussion about patient satisfaction in rehabilitation services. | High level of satisfaction with rehabilitation services |
|
36 | Ware et al (1983) Defining and measuring patient satisfaction with medical care. Evaluation and Planning Program Care Journal, 6 3-4, 246-253. | 55 Likert-type survey measuring patient satisfaction analysed | Describe the patient satisfaction questionnaire and test validity and reliability | Measured variables of customer care |
|
37 | Kupfer and Bond.(2012) Patient Satisfaction and Patient-Centered Care Necessary but Not Equal JAMA (2012), 3, 8, 139-40 | None | Viewpoint | States that patient satisfaction is not the same as patient-centred care. Suggest patient satisfaction is not always guaranteed by patient-centred care |
|
38 | William’s (1994) Patient satisfaction, a valid concept? Social Science and Medicine, 3, 516-23. | None | Review of literature | Presents satisfaction as a complex concept as the extent to be measured depends on the extent to be defined |
|
39 | Turris,(2005) Unpacking a patient’s concept of satisfaction- a feminist perspective. Journal of Advanced Nursing 50, 3, 293-298 | None | Review of literature | A feminist critique of patient satisfaction |
|
40 | Kaba and Soronkabium, (2007) The evolution of the doctor-patient relationship. International Journal Surgery, 4, 44-67. | None | Literature review | The need for ever-great progress toward a patient-centred approach |
|
41 | Rao et al.(2006) Toward patient-centred care in India- a scale to measure patients’ perception of quality. International Journal for the Quality of Care, 414-21. | 1869 Outpatients and 611 Inpatients were sampled from 4 different healthcare facilities in India | Cross-sectional survey | Measures of Perceived quality included: medicine availability, medical information, staff behaviour, doctor behaviour, and hospital infrastructure. |
|
42 | McCormack et al. (2011), Measuring patient-centred communication in cancer care: A literature review and the development of a systematic approach, Social Science & Medicine, Vol. 72, pp 1085-1095 | None | Literature review | Identified Six core concepts related to Patient-clinician communication as a critical element of patient-centred care |
|
43 | Jagosh et al. (2011), The importance of physician listening from the patients’ perspective: Enhancing diagnosis, healing, and the doctor-patient relationship, Patient Education and Counselling, Vol. 85, pp 369–374 | 58 Patients from McGill University Health Centre in Canada | Qualitative interpretive study | Three main themes were identified on why doctor listening is important to patients)essential components of clinical data gathering, 2) listening as a healing and therapeutic agent,3) fostering the doctor-patient relationship |
|
44 | Jackson et al. (2001), Predictors of patient satisfaction, Social Science and Medicine, Vol. 52, pp 609-620 | Patient survey of their satisfaction. A sample of 500 adults with physical symptoms attended a general medicine clinic in the USA | Cohort study | Satisfaction is influenced by personal characteristics and by the time frame immediately reported after the clinic visit 52% of them were satisfied while those 2 weeks after the visit 59 % of them were satisfied and 3 months after the visit 65 % of satisfied |
|
45 | Ong et al. (1995) Doctor-Patient Communication: A review of the literature. Social Science and Medicine, 40, 903-918. | None | Literature review | Synthesis of the existing literature on patient-doctor communication. It is central to a good relationship and health outcome |
|
46 | Holmström and Roing (2010). The relation between patient-centeredness and patient empowerment: A discussion on concepts. Patient Education and Counselling. 79(2), pp.167-172. | Concept analysis approach compared to literature review | Patient-centeredness and empowerment are complementary to each other. Patient empowerment can also be achieved by patient-centeredness |
|
47 | Roter (2000). The enduring and evolving nature of the patient-physician relationship. Patient Education and Counselling. 39, pp. 5-15 | NONE | Review of literature | Exploring relationship-centred medical paradigm on the nature of doctor-patient relationship. Thus, suggested a framework Linking therapeutics relationship to communication in the doctor-patient relationship |
|
48 | McWilliam et al (2000), Breast cancer patients’ experiences of patient-doctor communication: a working relationship, Patient Education and Counselling, Vol. 39, pp 191-204 | 11 Women with breast cancer interviewed | Qualitative phenomenological study | Identify the importance of patient patient-centred, working relationship. Effective communication as affective, behavioural and instrumental was linked to positive experiences of women with breast cancer |
|
49 | Shaw et al (2007), Doctor-patient relationship as motivation and outcome: Examining uses of an Interactive Cancer Communication System, International Journal of Medical Informatics, Vol. 76, pp 274-282 | 231 breast cancer patients given computer and access to internet information resources | Survey data collected pre-test and 4 months post the use of information system through the internet | Positive perception of doctor-patient relationship post-test. It is evident that information resources through the Internet do improve patient satisfaction |
|
50 | Kenny et al. (2010), Interpersonal perception in the context of doctor-patient relationships: A dyadic analysis of doctor-patient communication, Social Science & Medicine, Vol. 70, pp 763-768 | 91 doctors and 1749 patients in Canada | Cross-sectional study Doctors and patients independently completed questions on doctor communication skills after consultation visit | Doctors and patients had different views and perspectives on communication held during the consultation |
|
51 | Michie et al. (2003), Patient-centeredness in chronic illness: what is it and does it matter? Patient Education and Counselling, Vol 51, pp 197-206 | None | Review of literature They review 2 types of communication in chronic illness patient – patient activation and taking patient perspective and if it affects health outcomes | Activation of patients results in, good physical health outcomes more than taking only the patient's perspective. Therefore different types of patient-centred communication result in different health outcomes |
|
52 | Donabedian, (1980). Explorations in quality assessment and monitoring. Vol. 1. The definition of quality and approaches to its assessment. Ann Arbor, Mich.: Health Administration Press | None | Review | A proposed model to determine patient satisfaction with quality of care. Three domains which are structure, process and outcome can be used to define quality |
|
53 | Khamis, & Njau (2014).Patients' level of satisfaction with the quality of health care at Mwananyamala Hospital in Dar es Salaam, Tanzania. BMC health services research, 14(1), pp. 400-407 | a SEQUAL Questionnaire was used to collect data from 420 patients in an outpatient clinic in Tanzania | Cross-sectional survey study | The use of the Donabedian model to assess the level of patient satisfaction with the quality of care proves useful Poor satisfaction among patients generally because of a lack of communication |
|
54 | DuFrene R., (2000), An evaluation of a patient satisfaction survey: validity and reliability, Evaluation and Program Planning, Vol. 23, pp 293-300 | None | Comparative analysis | Testing the validity of external patient satisfaction surveys. They were often unreliable because of issues of poor design |
|
55 | Street et al. (2009). How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Education and Counselling. 74(3), pp. 295-301. | None | Literature review | Identified Seven pathways of communication to improve health | · The results imply the need for taking a patient-centred approach in communication to improve health as proposed by the Institute of Medicine's definition of patient-centeredness |
56 | Mead, and Bower, (2000). Patient-centeredness: A conceptual framework and review of the empirical literature. Social Science and Medicine. 51(7), pp 1087-1110. | None | Literature review | Five conceptual dimensions were identified to support patient centred model in doctor-patient relationships | · The findings cannot be generalized as patient-centred care depends mainly on sociocultural aspects of the setting and the applicability of the 5 dimensions identified needs to be tested in other cultural settings like KSA |
57 | Merkouris et al. (2004). Evaluation of patient satisfaction with nursing care: Quantitative or qualitative approach? International Journal of Nursing Studies. 41(4), pp. 355-367. | 200 Inpatients from 2 large hospitals in Greek | Mixed methods study (Quantitative and Qualitative methods concurrently for Triangulation ) | Patient satisfaction with nursing care was highly scored for technical competence while low scores were associated with information provision. Interpersonal aspects were central to the patient experience |
|
58 | Oberst (1983) ‘Patients perceptions of care’. Measurement of satisfaction. Cancer, 53, 2333-2337 | None | Discussion Paper on the nature of patient satisfaction in an Oncology setting. | Philosophical problems of subjective feeling of satisfaction |
|
Appendix 6: Participant information sheet (patients)
Study Title: Patient Satisfaction in Oncology Ward Settings in Saudi Arabia: A Mixed Methods Study
Project Investigator: Manal Banaser Contact Number: (number given)
Dear Participants
I would like to invite you to participate in a research study. Before you agree to participate, you need to understand the reason for the current study and what it will involve to make an effective contribution to the study field. Please read the below information about the study. Feel free to ask about any of the information and if you need even more information you can contact me any time at the above given contact number.
The study is a postgraduate research student project which is supervised by Dr Kathleen Stoddart and Dr Nicola Cunningam at the Department of Nursing, Midwifery and Health at the University of Stirling in the United Kingdom. This project is funded by the King Fahd Medical City Scholarships department in Riyadh.
Project Aim: The project is aimed to help understand the experience of adult hospitalised cancer patients with the received care by taking patient perspectives on doctors’ and nurses’ technical skills, information provision, availability and services organisation to make recommendations for improvement. The research study will be conducted in two phases. First, a questionnaire on patient satisfaction with care will be distributed to adult hospitalised cancer patients in a Saudi Regional Cancer Centre in Riyadh. Second, 6 participants of those who completed the questionnaire will be invited voluntarily to attend an individual interview with the research investigator to expand our knowledge of optimising satisfaction with care or making recommendations for areas of improvement in quality of care.
Advantages of taking part in the current study:
Your expectations and opinions for the received care in an oncology setting are an important aspect in ensuring quality of care. Your satisfaction scores will help healthcare providers to identify areas for improvement, as well as to maintain the quality of care in the future. By giving reasons for either satisfaction or dissatisfaction with care within the interviews, healthcare providers can have more understanding of their experiences with hospital care and eventually will make an effort to contribute to delivering effective, high-quality cancer services in Saudi Arabia.
In the first phase, you will have to complete the questionnaire by rating the aspects of care that were given in the hospital and then return it to the investigator. In the second phase, you will be invited to attend an interview with the researcher. You will be asked about the reasons for your satisfaction with care or the reasons if you are not satisfied. It will use open-ended questions and it might be recorded if you agree to maintain the accuracy of the results.
Participation in both phases of this project is voluntary. You may withdraw at any time with no consequences Please note, if you are interested in joining an interview for the second phase of the current study, you can contact me as early as possible.
Confidentiality
Confidentiality will be maintained by providing identification numbers rather than participant names for both questionnaire and interview records or notes. This will enhance the confidentiality of provided information. All records, notes of interviews, and answered questionnaires will be kept by the researcher in a secure place during the study period. Once the data have been analysed and the study completed, the information will be destroyed. Two supervisors will monitor the study and the findings will be written up as a Ph.D. thesis. You will not be identified at any stage of the written report or the thesis. All information will be kept anonymous, known only to the researcher and her supervisors. This project has been cleared by the University of Stirling Ethics Committee, as well as approved by the Ethics Committee of the Saudi Regional Cancer Centre in Riyadh.
Thank you for taking the time to read this information sheet and thinking about participation in the study.
Researcher Name: Manal Banaser Contact Number: (number provided)
Principal Supervisor: Dr. Kathleen Stoddart
Appendix 7: Patient consent form
Study Phase:
Participant identification number:
Study Title: Patient Satisfaction in Oncology Ward Settings in Saudi Arabia: A Mixed Methods Study
Researcher Name: Manal Banaser
I have read and understand the study information sheet and this consent form. I have had an opportunity to ask questions about my participation.
I understand that I am under no obligation to take part in the current study.
I understand that I have the right to withdraw from the current study at any stage without giving any reason.
I agree to participate in the current study.
Name of Participant:
Signature of Participant:
Signature of Researcher:
Date:
Contact details of the researcher
Name: Manal Banaser
Address: (address given)
Telephone Number: (number given)
Email: (address given)
Reference:
University of Stirling Research Ethics Committee. Informed consent. Available from: http://www.goodresearchpractice.stir.ac.uk/documents/Chapter6.pdf
Appendix 8: Recruitment log for patients
Study Title: Patient Satisfaction in oncology ward settings in Saudi Arabia: A mixed methods study
Name of Researcher: Manal Banaser
Patient ID | Age | Gender | Date of admission | Yes/No to study | Reason for admission | Date recruited | Date of data collection |
Appendix 9: EORCT inpatient satisfaction questionnaire EORTC IN-PATSAT32
We are interested in some things about you and your experience of the care received during your hospital stay. Please answer all the questions yourself by circling the number that best applies to you. There are no 'right' or 'wrong' answers. The information that you provide will remain strictly confidential.
During your hospital stay, how would you rate doctors, in terms of:
Poor, Fair, Good, Very good, Excellent
Questionnaire Item | Poor | Fair | Good | Very good | Excellent |
1 Their knowledge and experience of your illness? | 1 | 2 | 3 | 4 | 5 |
2 The treatment and medical follow-up do they provide? | 1 | 2 | 3 | 4 | 5 |
3 The attention they paid to your physical problems? | 1 | 2 | 3 | 4 | 5 |
4 Their willingness to listen to all of your concerns? | 1 | 2 | 3 | 4 | 5 |
5 The interest they show in you? | 1 | 2 | 3 | 4 | 5 |
6 The comfort and support they gave you? | 1 | 2 | 3 | 4 | 5 |
7 The information they gave you about your illness? | 1 | 2 | 3 | 4 | 5 |
8 The information they give you about your medical tests? | 1 | 2 | 3 | 4 | 5 |
9 The information they gave you about your treatment? | 1 | 2 | 3 | 4 | 5 |
10 The frequency of their visits/consultations? | 1 | 2 | 3 | 4 | 5 |
11 The time they devoted to you during visits/consultations? | 1 | 2 | 3 | 4 | 5 |
During your hospital stay, how would you rate nurses, in terms of:
Poor, Fair, Good, Very good, Excellent
Questionnaire Item | Poor | Fair | Good | Very good | Excellent |
12 The way they carried out your physical examination (took your temperature, felt your pulse,…)? | 1 | 2 | 3 | 4 | 5 |
13 The way they handled your care (gave your medicines, performed injections,…)? | 1 | 2 | 3 | 4 | 5 |
14 The attention they paid to your physical comfort? | 1 | 2 | 3 | 4 | 5 |
15 The interest they showed in you? | 1 | 2 | 3 | 4 | 5 |
16 The comfort and support they gave you? | 1 | 2 | 3 | 4 | 5 |
Please go on to the next page
During your hospital stay, how would you rate nurses, in terms of:
Poor, Fair Good, Very Good, Excellent
Questionnaire Item | Poor | Fair | Good | Very good | Excellent |
17 Their human qualities (politeness, respect, Sensitivity, kindness, patience,…)? | 1 | 2 | 3 | 4 | 5 |
18 The information they gave you about your medical tests? | 1 | 2 | 3 | 4 | 5 |
19 The information they gave you about your care? | 1 | 2 | 3 | 4 | 5 |
20 The information they gave you about your treatment? | 1 | 2 | 3 | 4 | 5 |
21 Their promptness in answering your buzzer calls? | 1 | 2 | 3 | 4 | 5 |
22 The time they devoted to you? | 1 | 2 | 3 | 4 | 5 |
During your hospital stay, how would you rate services and care organisation, in terms of Poor, Fair, Good, Very good, Excellent
Questionnaire Item | Poor | Fair | Good | Very good | Excellent |
23 The exchange of information between caregivers? | 1 | 2 | 3 | 4 | 5 |
24 The kindness and helpfulness of the technical, reception, and laboratory personnel? | 1 | 2 | 3 | 4 | 5 |
25 The information provided on your admission to the hospital? | 1 | 2 | 3 | 4 | 5 |
26 The information provided on your discharge from the hospital? | 1 | 2 | 3 | 4 | 5 |
27 The waiting time for obtaining results of medical tests? | 1 | 2 | 3 | 4 | 5 |
28 The speed of implementing medical tests and/or treatments? | 1 | 2 | 3 | 4 | 5 |
29 The ease of access (parking, means of transport…)? | 1 | 2 | 3 | 4 | 5 |
30 The ease of finding one’s way to the different departments? | 1 | 2 | 3 | 4 | 5 |
31 The environment of the building (cleanliness, calmness….)? | 1 | 2 | 3 | 4 | 5 |
In general
Questionnaire Item | Poor | Fair | Good | Very good | Excellent |
32 How would you rate the care received during your hospital stay? | 1 | 2 | 3 | 4 | 5 |
© QLQ-IN-PATSAT32 Copyright 2001 EORTC Quality of life Group. All rights reserved. Permission granted through EORCT email
DEMOGRAPHIC QUESTIONNAIRE ( Quantitative Phase 1 )
- Age
- From 18-25Years old
- From 26-35 Years old
- From 36-45 Years old
- From 46-55 Years old
- From 56-65 Years old
- From 66-75 Years old
- Above 76 Years old
- Gender
- Male
- Female ¨
- Marital status
- Single ¨
- Married ¨
- Divorced ¨
- Widowed ¨
- Education level
- Primary ¨
- Intermediate ¨
- High ¨
- University degree – above ¨
- Illiterate ¨
- Place of Residence
- Riyadh ¨
- Outside Riyadh ¨
Appendix 10: A Scoring Manual for in-patient Satisfaction Questionnaire
Scoring Procedure for the EORTC IN-PATSAT32
[Reference: Brédart et al, EJC, 41 (2005) 2120-2131]
The international field-testing study of the EORTC cancer in-patient satisfaction with care measure (EORTCIN-PATSAT32) has confirmed the hypothetical structure of the questionnaire. This questionnaire should thus be scored as follows:
1) Content of the questionnaire
Multi-item scales
- Doctors
Interpersonal skills (items 4-6)
Technical skills (items 1-3)
Information provision (items 7-9)
Availability (items 10, 11)
- Nurses
Interpersonal skills (items 15-17)
Technical skills (items 12-14)
Information provision (items 18-20)
Availability (items 21, 22)
- Other hospital personnel kindness and helpfulness, and information giving (24-26)
- Waiting time (performing medical tests/treatment, receiving medical test results) (items 27, 28)
- Access (items 29, 30)
Single item scale
- Exchange of information (item 23)
- Comfort/cleanness (item 31)
- General satisfaction (item 32)
2) Format of the questionnaire
Period of reference: Refer to interactions with health care providers and services in the oncology hospital during hospital stay.
How would you rate it? Poor (1)/Fair (2)/Good (3)/Very Good (4)/Excellent (5)
Number of items: 32
3) Scoring procedure
All multi-item or single-item scales are all constructed similarly: (1) the raw scores for the individual items within a scale are first summed, and then, for the multi-item scales, divided by the number of items in the scale; and (2) these scale scores are then linearly transformed such that all scales range from 0 to 100, with a
higher scale score representing a higher level of satisfaction with care.
Scoring details
In the 32-item questionnaire, each response is given a numerical equivalent (poor=1, excellent=5). Scores for each of the fourteen subscales of the questionnaire will first be determined for each patient. All the scores for all items in a particular subscale are summed, and then divided by the number of items in that subscale. For example, for doctors’ technical skills, the patients’ responses on items 1, 2 and 3 are added together, and then divided by 3. The scale scores are then linearly transformed to a 0-100 scale with a high score reflecting a higher level of satisfaction. So, for example, the items relating to satisfaction with doctors’ technical skills are questions 1, 2 and 3. If a participant answered with a rating of 3, 4, and 4 for those questions, the scores would be summed (=11), then divided by 3 (=3.67). To linearly transform the data to a scale ranging from 0-100, that score will be divided by 5 (highest possible score) and multiplied by 100 (in this case 3.67/5 = .7333 * 100 = 73.33).
Get 3+ Free Dissertation Topics within 24 hours?